

Association of Neurocognitive Deficits With Radiotherapy or Chemoradiotherapy for Patients With Head and Neck Cancer
- PMID: 29167901
- PMCID: PMC5833597
- DOI: 10.1001/jamaoto.2017.2235
Association of Neurocognitive Deficits With Radiotherapy or Chemoradiotherapy for Patients With Head and Neck Cancer
Abstract
Importance: Neurocognitive deficits (NCD) have been observed in noncentral nervous system cancers, yet short- and long-term neurocognitive data on patients treated for head and neck cancer (HNC) are lacking.
Objective: To assess objective neurocognitive function before and after definitive radiation therapy for HNC.
Design, setting, and participants: In a prospective, longitudinal study, neurocognitive function and self-reported symptoms were assessed in 80 patients with histologically proven HNC requiring definitive chemoradiotherapy or radiotherapy and in 40 healthy controls 4 times (baseline, 6, 12, and 24 months after baseline) prior to commencing treatment at Princess Margaret Cancer Centre, Toronto, Canada.
Main outcomes and measures: Neurocognitive test scores were converted to age-corrected z scores (mean, 0; standard deviation, 1) and reported as mean scores, standardized regression-based scores, and frequencies of impairments in intellectual capacity, concentration, memory, executive function, processing speed, and motor dexterity. Multivariable analysis was used to identify factors associated with NCD 2 years after treatment.
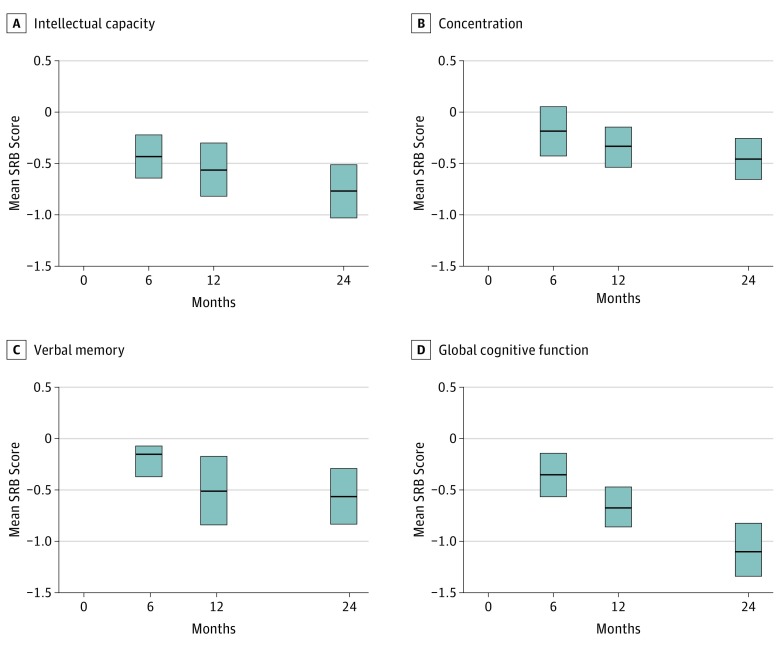
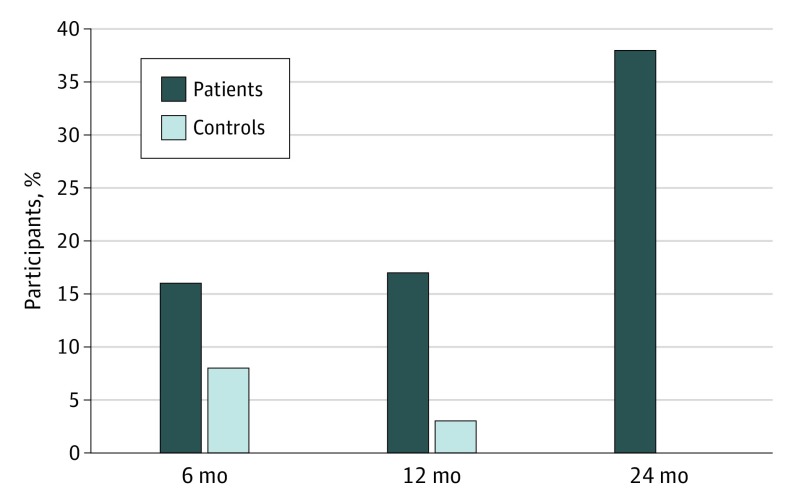
Results: Eighty patients and 40 healthy controls enrolled. Analyses revealed significant differences between patient and control mean performance in some domains, with patient deficits increasing over time: intellectual capacity (Cohen d, effect sizes [95% CIs] of -0.46 [-0.64 to 0.30], -0.51 [-0.72 to -0.30], and -0.70 [-0.92 to -0.49] for time points 6, 12, and 24 months, respectively); concentration/short-term attention span (-0.19 [-0.37 to 0.00], -0.38 [-0.55 to -0.21], -0.54 [-0.71 to -0.37]); verbal memory (-0.16 [-0.33 to 0.02], -0.38 [-0.64 to -0.12], -0.53 [-0.74 to -0.32]); executive function (-0.14 [-0.27 to 0.00], -0.34 [-0.52 to -0.16], -0.43 [-0.64 to -0.22]), and global cognitive function composite (-0.38 [-0.55 to -0.22], -0.75 [-0.92 to -0.58], -1.06 [-1.26 to -0.86]). There was an increased rate of impaired global neurocognitive functioning among patients (38%) at 24 months compared with controls (0%). Neurocognitive deficits were not associated with baseline cytokines.
Conclusions and relevance: Head and neck cancer survivors have neurocognitive sequelae up to 2 years after definitive chemoradiotherapy or radiation treatment. Patients and health care teams should know about such potential risks. Further research is warranted in search of strategies to avoid, reduce, and compensate for declines.
Conflict of interest statement
Figures
References
-
- Klein M, Heimans JJ, Aaronson NK, et al. . Effect of radiotherapy and other treatment-related factors on mid-term to long-term cognitive sequelae in low-grade gliomas: a comparative study. Lancet. 2002;360(9343):1361-1368. - PubMed
-
- Edelstein K, D’agostino N, Bernstein LJ, et al. . Long-term neurocognitive outcomes in young adult survivors of childhood acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2011;33(6):450-458. - PubMed
-
- Stewart A, Bielajew C, Collins B, Parkinson M, Tomiak E. A meta-analysis of the neuropsychological effects of adjuvant chemotherapy treatment in women treated for breast cancer. Clin Neuropsychol. 2006;20(1):76-89. - PubMed
-
- Bernstein LJ, Catton PA, Tannock IF. Intra-individual variability in women with breast cancer. J Int Neuropsychol Soc. 2014;20(4):380-390. - PubMed
-
- Edelstein K, Bernstein LJ. Cognitive dysfunction after chemotherapy for breast cancer. J Int Neuropsychol Soc. 2014;20(4):351-356. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
