

No advantage of fresh blastocyst versus cleavage stage embryo transfer in women under the age of 39: a randomized controlled study
- PMID: 29168022
- PMCID: PMC5904063
- DOI: 10.1007/s10815-017-1092-2
No advantage of fresh blastocyst versus cleavage stage embryo transfer in women under the age of 39: a randomized controlled study
Abstract
Purpose: Is there a difference in implantation and pregnancy rates between embryos transferred electively at cleavage or blastocyst stage in infertile women ≤ 38 years with at least four zygotes on day 1 post retrieval?
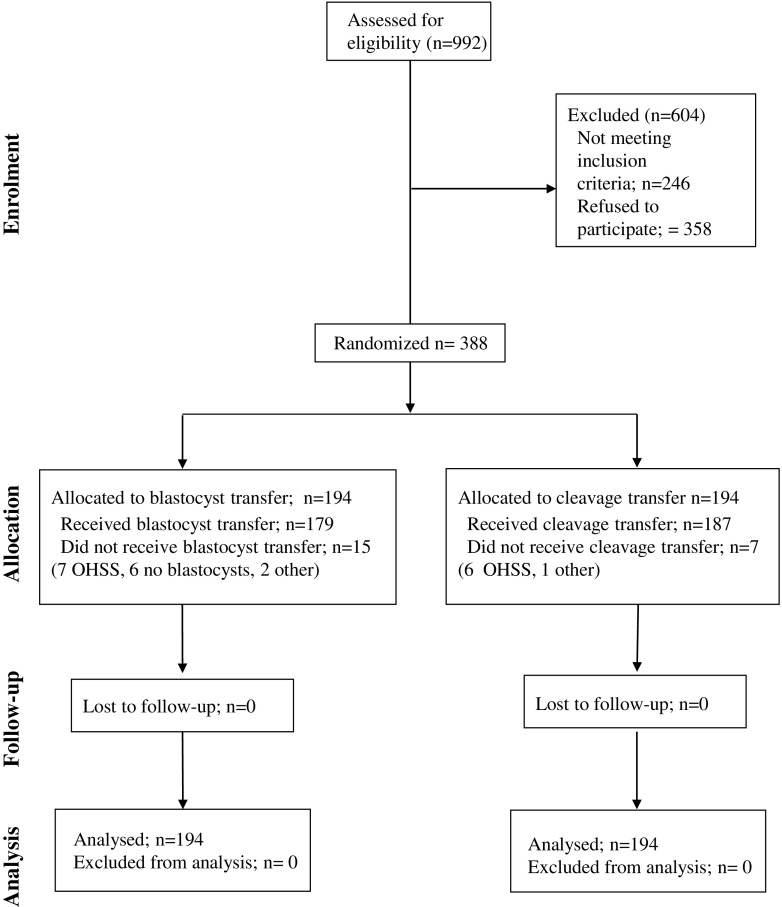
Methods: A randomized clinical trial was conducted in a single tertiary care hospital with a sample size of 194 patients in each arm for a total population of 388 women. Patients less than 39 years of age with more than three fertilized oocytes and less than four previous assisted reproductive technology (ART) attempts were inclusion criteria.
Results: The two groups were similar for age, years of infertility, indication to treatment, basal antimüllerian hormone and FSH, number of previous ART cycles, primary or secondary infertility, type of induction protocol, days of stimulation, total gonadotrophin dose, and estradiol (E2) and progesterone (P) levels at trigger. No statistically significant differences were found in terms of number of retrieved oocytes, inseminated oocytes, fertilization rate, canceled transfers (7.73% in blastocyst and 3.61% in cleavage stage group), and cycles with frozen embryos and/or oocytes. Although a higher number of fertilized oocytes were in the blastocyst stage group (6.18 ± 1.46 vs 5.89 ± 1.54, p = 0.052), a statistically greater number of embryos/randomized cycle were transferred at cleavage stage (1.93 ± 0.371) compared with the number of transferred blastocysts (1.80 ± 0.56), probably due to the number of embryos not reaching blastocyst stage (3.09%). The implantation rate (28.37 vs 25.67%), pregnancy rate per cycle (36.06 vs38.66%), transfer (39.66 vs 40.11%), spontaneous abortions (19.72% vs 12.00%), delivery rate per cycle (27.84 vs 32.99%), and transfer (30.17 vs 34.22%) were not significantly different between the blastocyst and cleavage stage groups. The twin delivery rate was higher in the blastocyst stage group, although not significant (42.59 vs 28.12%). The mean numbers of frozen blastocyst (2.30 ± 1.40 vs 2.02 ± 1.00) and frozen oocytes (7.09 ± 3.55vs 6.79 ± 3.26) were not significantly different between the two groups.
Conclusions: Fresh blastocyst-stage transfer versus cleavage-stage transfer did not show any significant difference in terms of implantation and pregnancy rate in this selected group of patients. A high twin delivery rate in both groups (35.59%) was registered, and although not significant, they were higher in the blastocyst transfer group (42.59 vs 28.12%). Our conclusion supports considering single embryo transfer (SET) policy, even in cleavage stage in patients younger than 39 years with at least four zygotes.
Trial registration: ClinicalTrials.gov registration number NCT02639000.
Keywords: Blastocyst stage; Cleavage stage; Cost-effectiveness; IVF/ICSI; Prediction models.
Conflict of interest statement
The study protocol and specific consent form have been approved by our Ethical Committee on June 24, 2010.
ᅟ
Conflict of interest
The authors declare that they have no conflict of interest.
References
-
- Human Fertilisation and Embryology Authority. Fertility treatment 2014 – Trends and figures. In. www.hfea.gov.uk. 2009–2010.
-
- Glujovsky D, Farquhar C, Quinteiro Retamar AM, Alvarez Sedo CR, Blake D. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. Cochrane Database Syst Rev 2016;(6):CD002118. 10.1002/14651858.CD002118.pub5. - PubMed
-
- Capalbo A, Rienzi L, Cimadomo D, Maggiulli R, Elliott T, Wright G, et al. Correlation between standard blastocyst morphology, euploidy and implantation: an observational study in two centers involving 956 screened blastocysts. Hum Reprod. 2014; - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
