

Gating the holes in the Swiss cheese (part I): Expanding professor Reason's model for patient safety
- PMID: 29168290
- PMCID: PMC5901035
- DOI: 10.1111/jep.12847
Gating the holes in the Swiss cheese (part I): Expanding professor Reason's model for patient safety
Abstract
Introduction: Although patient safety has improved steadily, harm remains a substantial global challenge. Additionally, safety needs to be ensured not only in hospitals but also across the continuum of care. Better understanding of the complex cognitive factors influencing health care-related decisions and organizational cultures could lead to more rational approaches, and thereby to further improvement.
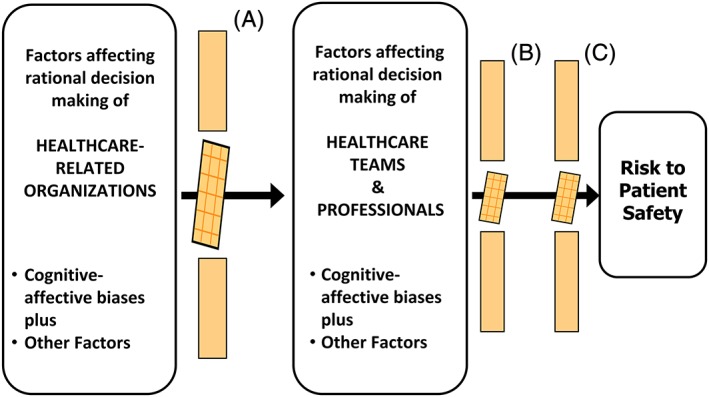
Hypothesis: A model integrating the concepts underlying Reason's Swiss cheese theory and the cognitive-affective biases plus cascade could advance the understanding of cognitive-affective processes that underlie decisions and organizational cultures across the continuum of care.
Methods: Thematic analysis, qualitative information from several sources being used to support argumentation.
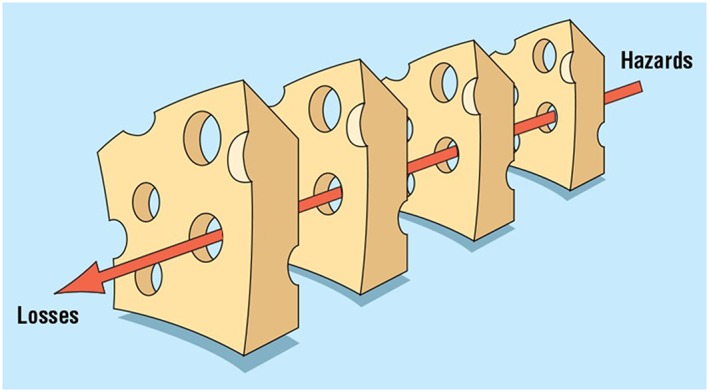
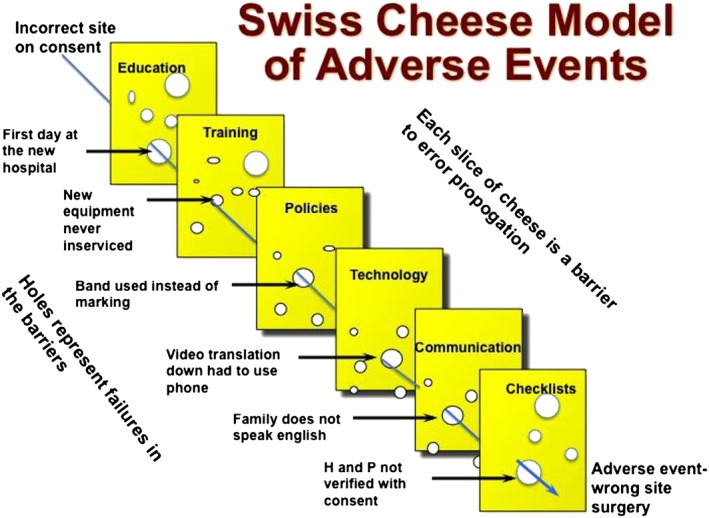
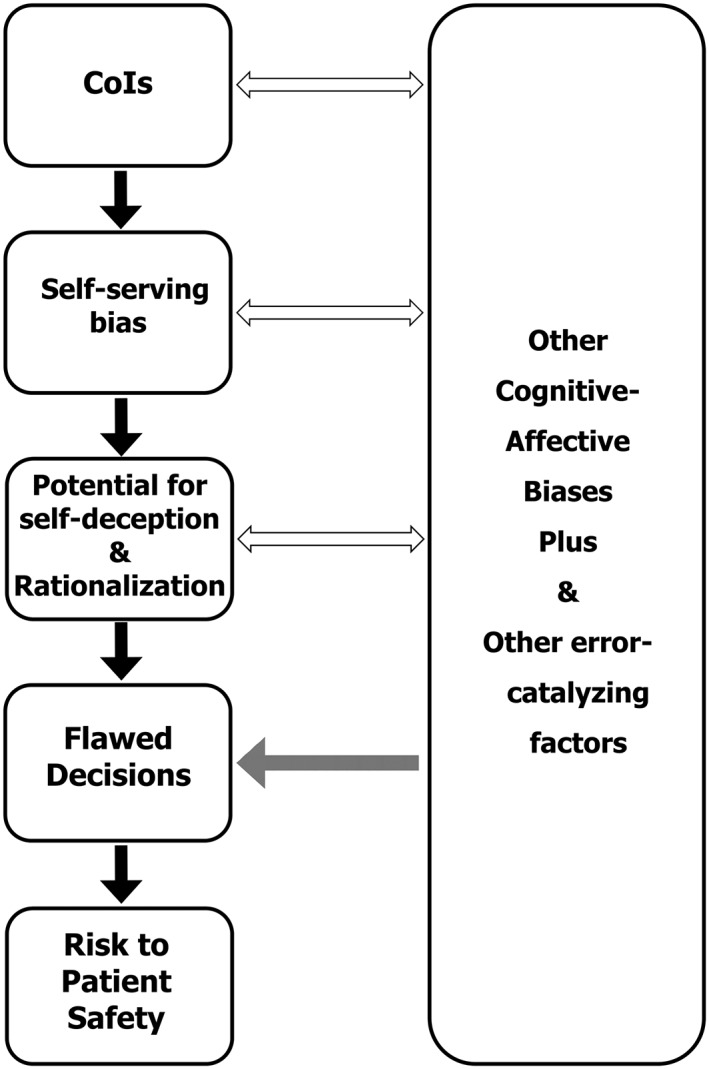
Discussion: Complex covert cognitive phenomena underlie decisions influencing health care. In the integrated model, the Swiss cheese slices represent dynamic cognitive-affective (mental) gates: Reason's successive layers of defence. Like firewalls and antivirus programs, cognitive-affective gates normally allow the passage of rational decisions but block or counter unsounds ones. Gates can be breached (ie, holes created) at one or more levels of organizations, teams, and individuals, by (1) any element of cognitive-affective biases plus (conflicts of interest and cognitive biases being the best studied) and (2) other potential error-provoking factors. Conversely, flawed decisions can be blocked and consequences minimized; for example, by addressing cognitive biases plus and error-provoking factors, and being constantly mindful. Informed shared decision making is a neglected but critical layer of defence (cognitive-affective gate). The integrated model can be custom tailored to specific situations, and the underlying principles applied to all methods for improving safety. The model may also provide a framework for developing and evaluating strategies to optimize organizational cultures and decisions.
Limitations: The concept is abstract, the model is virtual, and the best supportive evidence is qualitative and indirect.
Conclusions: The proposed model may help enhance rational decision making across the continuum of care, thereby improving patient safety globally.
Keywords: cognition; cognitive biases; evidence-based medicine; gate model; healthcare; organizations; patient safety; rational decision making.
© 2017 The Authors. Journal of Evaluation in Clinical Practice published by John Wiley & Sons, Ltd.
Figures
Similar articles
-
Hot cheese: a processed Swiss cheese model.J R Coll Physicians Edinb. 2014;44(2):116-21. doi: 10.4997/JRCPE.2014.205. J R Coll Physicians Edinb. 2014. PMID: 24999771
-
Evidence-informed person-centered healthcare part I: do 'cognitive biases plus' at organizational levels influence quality of evidence?J Eval Clin Pract. 2014 Dec;20(6):734-47. doi: 10.1111/jep.12280. Epub 2014 Nov 28. J Eval Clin Pract. 2014. PMID: 25429739 Review.
-
The Swiss cheese model of safety incidents: are there holes in the metaphor?BMC Health Serv Res. 2005 Nov 9;5:71. doi: 10.1186/1472-6963-5-71. BMC Health Serv Res. 2005. PMID: 16280077 Free PMC article.
-
The patient experience of patient-centered communication with nurses in the hospital setting: a qualitative systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):76-87. doi: 10.11124/jbisrir-2015-1072. JBI Database System Rev Implement Rep. 2015. PMID: 26447009
-
Effectiveness of the surgical safety checklist in correcting errors: a literature review applying Reason's Swiss cheese model.AORN J. 2014 Jul;100(1):65-79.e5. doi: 10.1016/j.aorn.2013.07.024. AORN J. 2014. PMID: 24973186 Review.
Cited by
-
Clinical reasoning in dire times. Analysis of cognitive biases in clinical cases during the COVID-19 pandemic.Intern Emerg Med. 2022 Jun;17(4):979-988. doi: 10.1007/s11739-021-02884-9. Epub 2022 Jan 8. Intern Emerg Med. 2022. PMID: 34997906 Free PMC article.
-
Fall risk factors and mitigation strategies for hematological malignancy patients: insights from a qualitative study using the reason model.Support Care Cancer. 2025 Jan 24;33(2):118. doi: 10.1007/s00520-025-09170-w. Support Care Cancer. 2025. PMID: 39849285
-
Nurses' perceptions of fall risk factors and fall prevention strategies in acute care settings in Saudi Arabia.Nurs Open. 2022 Mar;9(2):1362-1369. doi: 10.1002/nop2.1182. Epub 2022 Jan 30. Nurs Open. 2022. PMID: 35099122 Free PMC article.
-
Implicit bias in healthcare: clinical practice, research and decision making.Future Healthc J. 2021 Mar;8(1):40-48. doi: 10.7861/fhj.2020-0233. Future Healthc J. 2021. PMID: 33791459 Free PMC article.
-
"Incident Teaching (IT)" Lecture Series - Incorporating Education Surrounding Clinical Incidents and Complaints into Foundation Year 1 (FY1) Doctors' Induction.J Eur CME. 2021 Jan 19;10(1):1874643. doi: 10.1080/21614083.2021.1874643. J Eur CME. 2021. PMID: 33552678 Free PMC article.
References
-
- National Academies of Sciences, Engineering and Medicine . Improving diagnosis in health care. Washington, DC, USA: The National Academies Press; 2015.
-
- Saini V, Garcia‐Armesto S, Klemperer D, et al. Drivers of poor medical care. Lancet. 2017;390:178‐190. - PubMed
-
- Institute of Medicine (US) Committee on Quality of Health Care in America . To err is Human: Building a Safer Health System. Washington (DC): The National Academies Press; 2000. - PubMed
-
- Jha AK, Prasopa‐Plaizier N, Larizgoitia I, Bates DW. Research priority setting working group of the WHO world alliance for patient safety. Patient safety research: an overview of the global evidence. Qual Saf Health Care. 2010;19(1):42‐47. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
