

Social and clinical determinants of preferences and their achievement at the end of life: prospective cohort study of older adults receiving palliative care in three countries
- PMID: 29169346
- PMCID: PMC5701500
- DOI: 10.1186/s12877-017-0648-4
Social and clinical determinants of preferences and their achievement at the end of life: prospective cohort study of older adults receiving palliative care in three countries
Abstract
Background: Achieving choice is proposed as a quality marker. But little is known about what influences preferences especially among older adults. We aimed to determine and compare, across three countries, factors associated with preferences for place of death and treatment, and actual site of death.
Methods: We recruited adults aged ≥65-years from hospital-based multiprofessional palliative care services in London, Dublin, New York, and followed them for >17 months. All services offered consultation on hospital wards, support for existing clinical teams, outpatient services and received funding from their National Health Service and/or relevant Insurance reimbursements. The New York service additionally had 10 inpatient beds. All worked with and referred patients to local hospices. Face-to-face interviews recorded most and least preferred place of death, treatment goal priorities, demographic and clinical information using validated questionnaires. Multivariable and multilevel analyses assessed associated factors.
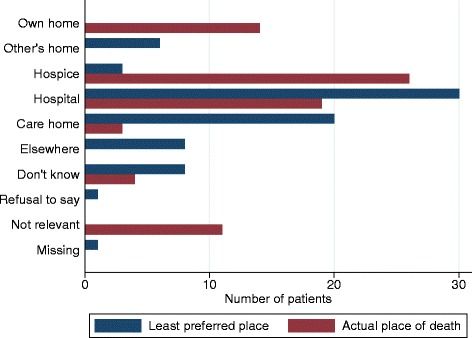
Results: One hundred and thirty eight older adults (64 London, 59 Dublin, 15 New York) were recruited, 110 died during follow-up. Home was the most preferred place of death (77/138, 56%) followed by inpatient palliative care/hospice units (22%). Hospital was least preferred (35/138, 25%), followed by nursing home (20%) and home (16%); hospice/palliative care unit was rarely least preferred (4%). Most respondents prioritised improving quality of life, either alone (54%), or equal with life extension (39%); few (3%) chose only life extension. There were no significant differences between countries. Main associates with home preference were: cancer diagnosis (OR 3.72, 95% CI 1.40-9.90) and living with someone (OR 2.19, 1.33-3.62). Adults with non-cancer diagnoses were more likely to prefer palliative care units (OR 2.39, 1.14-5.03). Conversely, functional independence (OR 1.05, 1.04-1.06) and valuing quality of life (OR 3.11, 2.89-3.36) were associated with dying at home. There was a mismatch between preferences and achievements - of 85 people who preferred home or a palliative care unit, 19 (25%) achieved their first preference.
Conclusion: Although home is the most common first preference, it is polarising and for 16% it is the least preferred. Inpatient palliative care unit emerges as the second most preferred place, is rarely least preferred, and yet was often not achieved for those who wanted to die there. Factors affecting stated preferences and met preferences differ. Available services, notably community support and palliative care units, require expansion. Contrasting actual place of death with capacity for meeting patient and family needs may be a better quality indicator than simply 'achieved preferences'.
Keywords: Ageing; Elderly; End-of-life care; Home; Hospice; Hospital; Palliative care; Place of death; Preferences.
Conflict of interest statement
Ethics approval and consent to participate
The study received ethical approval from the Research Ethics Committee in Dulwich, London in the UK (Ref. 12/LO/0044); the ethics committees of the Mater Misericordiae University Hospital (MMUH) and Beaumont Hospital in Ireland (Ref. 1/378/1456 and Ref. 12/07, respectively); and the Institutional Review Board of the Icahn School of Medicine at Mount Sinai in the USA (Ref. GCO#11–0845). Additionally, UK NHS research and development approval was received.
If participants were agreeable to being approached, a researcher fully explained the study to them, provided an information sheet and gained written informed consent. Adults unable to give informed consent or deemed too ill to complete any part of the interview were excluded.
Consent for publication
Not applicable
Competing interests
We declare no conflicts of or competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- NHS Finance and Operations/NHS Group/NHSCS/17189: Our commitment to you for end of life care. The government response to the review of choice in end of life care. London: UK Government, Crown copyright 2016. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil.... Accessed 28 Jul 2016.
-
- HOUSE OF REPRESENTATIVES (introduced by Blumenauer and Roe): H. R. 5555. Personalize your care act 2.0. Washington, DC: US Government; 2016. Available at: https://www.congress.gov/114/bills/hr5555/BILLS-114hr5555ih.xml. Accessed 28 Jul 2016.
-
- Cohen J, Pivodic L, Miccinesi G, Onwuteaka-Philipsen BD, Naylor WA, Wilson DM, Loucka M, Csikos A, Pardon K, Van den Block L et al: International study of the place of death of people with cancer: a population-level comparison of 14 countries across 4 continents using death certificate data. Br J Cancer 2015, 113(9):1397-1404. - PMC - PubMed
-
- Gao W, Ho YK, Verne J, Gordon E, Higginson IJ: Geographical and temporal understanding in place of death in England (1984–2010): analysis of trends and associated factors to improve end-of-life care (GUIDE_Care) - primary research. Southampton (UK): National Institutes for Health Research; 2014 (Health Services and Delivery Research, No. 2.42.). Available at: https://www.ncbi.nlm.nih.gov/books/NBK263581/. doi:10.3310/hsdr02420. Accessed 7 Jan 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
