

Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial
- PMID: 29169668
- PMCID: PMC5803129
- DOI: 10.1016/S0140-6736(17)32457-1
Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial
Abstract
Background: Arthroscopic sub-acromial decompression (decompressing the sub-acromial space by removing bone spurs and soft tissue arthroscopically) is a common surgery for subacromial shoulder pain, but its effectiveness is uncertain. We did a study to assess its effectiveness and to investigate the mechanism for surgical decompression.
Methods: We did a multicentre, randomised, pragmatic, parallel group, placebo-controlled, three-group trial at 32 hospitals in the UK with 51 surgeons. Participants were patients who had subacromial pain for at least 3 months with intact rotator cuff tendons, were eligible for arthroscopic surgery, and had previously completed a non-operative management programme that included exercise therapy and at least one steroid injection. Exclusion criteria included a full-thickness torn rotator cuff. We randomly assigned participants (1:1:1) to arthroscopic subacromial decompression, investigational arthroscopy only, or no treatment (attendance of one reassessment appointment with a specialist shoulder clinician 3 months after study entry, but no intervention). Arthroscopy only was a placebo as the essential surgical element (bone and soft tissue removal) was omitted. We did the randomisation with a computer-generated minimisation system. In the surgical intervention groups, patients were not told which type of surgery they were receiving (to ensure masking). Patients were followed up at 6 months and 1 year after randomisation; surgeons coordinated their waiting lists to schedule surgeries as close as possible to randomisation. The primary outcome was the Oxford Shoulder Score (0 [worst] to 48 [best]) at 6 months, analysed by intention to treat. The sample size calculation was based upon a target difference of 4·5 points (SD 9·0). This trial has been registered at ClinicalTrials.gov, number NCT01623011.
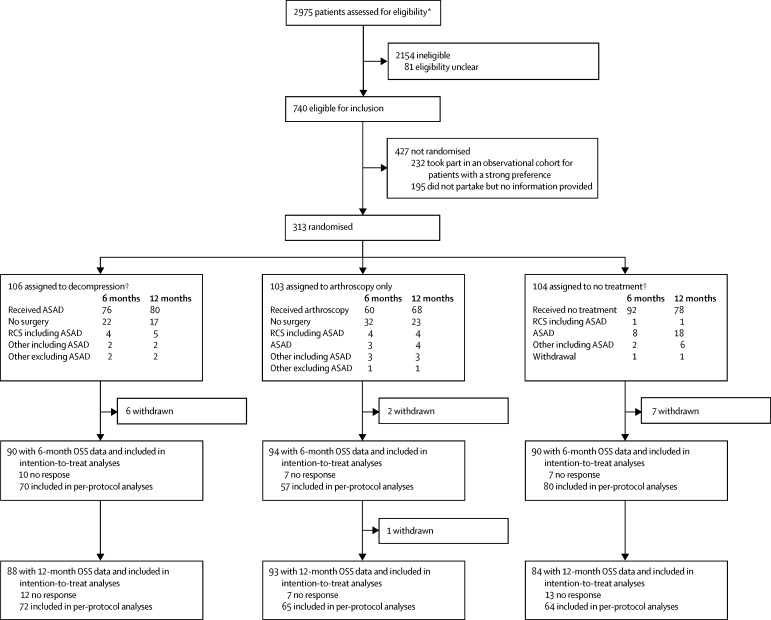
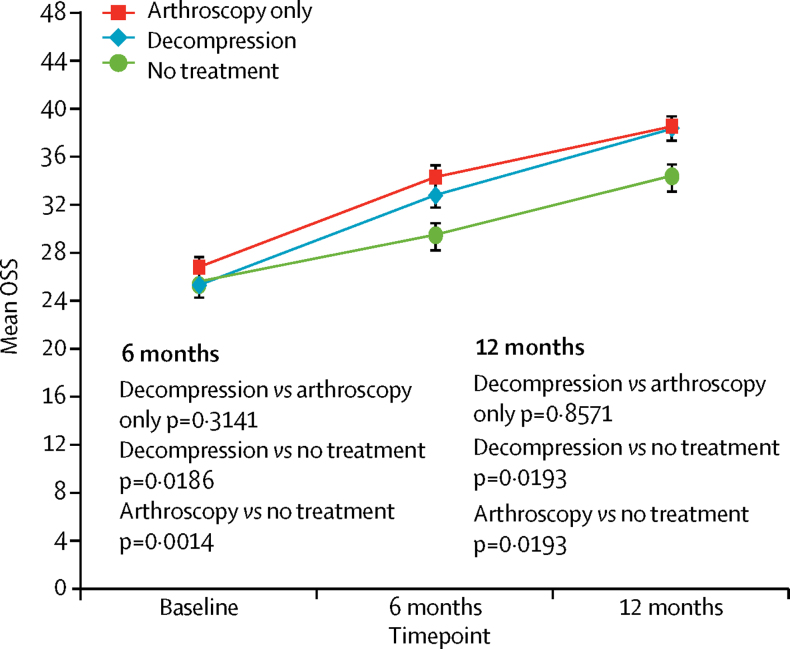
Findings: Between Sept 14, 2012, and June 16, 2015, we randomly assigned 313 patients to treatment groups (106 to decompression surgery, 103 to arthroscopy only, and 104 to no treatment). 24 [23%], 43 [42%], and 12 [12%] of the decompression, arthroscopy only, and no treatment groups, respectively, did not receive their assigned treatment by 6 months. At 6 months, data for the Oxford Shoulder Score were available for 90 patients assigned to decompression, 94 to arthroscopy, and 90 to no treatment. Mean Oxford Shoulder Score did not differ between the two surgical groups at 6 months (decompression mean 32·7 points [SD 11·6] vs arthroscopy mean 34·2 points [9·2]; mean difference -1·3 points (95% CI -3·9 to 1·3, p=0·3141). Both surgical groups showed a small benefit over no treatment (mean 29·4 points [SD 11·9], mean difference vs decompression 2·8 points [95% CI 0·5-5·2], p=0·0186; mean difference vs arthroscopy 4·2 [1·8-6·6], p=0·0014) but these differences were not clinically important. There were six study-related complications that were all frozen shoulders (in two patients in each group).
Interpretation: Surgical groups had better outcomes for shoulder pain and function compared with no treatment but this difference was not clinically important. Additionally, surgical decompression appeared to offer no extra benefit over arthroscopy only. The difference between the surgical groups and no treatment might be the result of, for instance, a placebo effect or postoperative physiotherapy. The findings question the value of this operation for these indications, and this should be communicated to patients during the shared treatment decision-making process.
Funding: Arthritis Research UK, the National Institute for Health Research Biomedical Research Centre, and the Royal College of Surgeons (England).
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
No benefit of arthroscopy in subacromial shoulder pain.Lancet. 2018 Jan 27;391(10118):289-291. doi: 10.1016/S0140-6736(17)32874-X. Epub 2017 Nov 20. Lancet. 2018. PMID: 29169667 No abstract available.
-
Can Shoulder Arthroscopy Work? (CSAW) trial.Lancet. 2018 Jul 28;392(10144):280-281. doi: 10.1016/S0140-6736(18)30778-5. Lancet. 2018. PMID: 30064648 No abstract available.
-
Can Shoulder Arthroscopy Work? (CSAW) trial.Lancet. 2018 Jul 28;392(10144):281. doi: 10.1016/S0140-6736(18)30777-3. Lancet. 2018. PMID: 30064649 No abstract available.
-
Can Shoulder Arthroscopy Work? (CSAW) trial - Authors' reply.Lancet. 2018 Jul 28;392(10144):281-282. doi: 10.1016/S0140-6736(18)30773-6. Lancet. 2018. PMID: 30064650 No abstract available.
-
The improper use of a no-treatment group in the randomised surgical trial for subacromial shoulder pain.Clin Exp Rheumatol. 2019 Nov-Dec;37 Suppl 122(6):9. Epub 2019 Nov 6. Clin Exp Rheumatol. 2019. PMID: 31694751 No abstract available.
-
Is acromioplasty justifiable?Orthop Traumatol Surg Res. 2019 Dec;105(8S):S199-S200. doi: 10.1016/j.otsr.2019.10.002. Epub 2019 Nov 4. Orthop Traumatol Surg Res. 2019. PMID: 31694802 No abstract available.
References
-
- Linsell L, Dawson J, Zondervan K. Prevalence and incidence of adults consulting for shoulder conditions in UK primary care; patterns of diagnosis and referral. Rheumatology. 2006;45:215–221. - PubMed
-
- Oh LS, Wolf BR, Hall MP, Levy BA, Marx RG. Indications for rotator cuff repair: a systematic review. Clin Orthop Relat Res. 2007;455:52–63. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
