

Comparison of the Between the Flags calling criteria to the MEWS, NEWS and the electronic Cardiac Arrest Risk Triage (eCART) score for the identification of deteriorating ward patients
- PMID: 29169912
- PMCID: PMC6556215
- DOI: 10.1016/j.resuscitation.2017.10.028
Comparison of the Between the Flags calling criteria to the MEWS, NEWS and the electronic Cardiac Arrest Risk Triage (eCART) score for the identification of deteriorating ward patients
Abstract
Introduction: Traditionally, paper based observation charts have been used to identify deteriorating patients, with emerging recent electronic medical records allowing electronic algorithms to risk stratify and help direct the response to deterioration.
Objective(s): We sought to compare the Between the Flags (BTF) calling criteria to the Modified Early Warning Score (MEWS), National Early Warning Score (NEWS) and electronic Cardiac Arrest Risk Triage (eCART) score.
Design and participants: Multicenter retrospective analysis of electronic health record data from all patients admitted to five US hospitals from November 2008-August 2013.
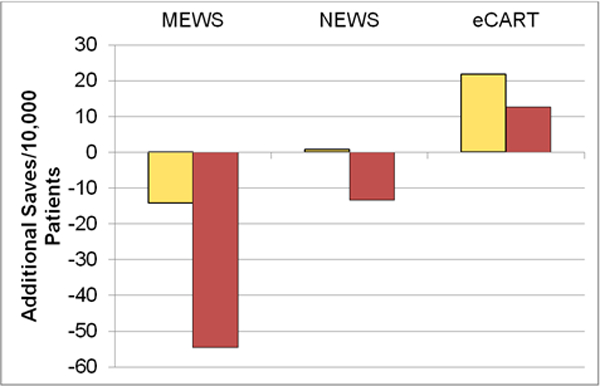
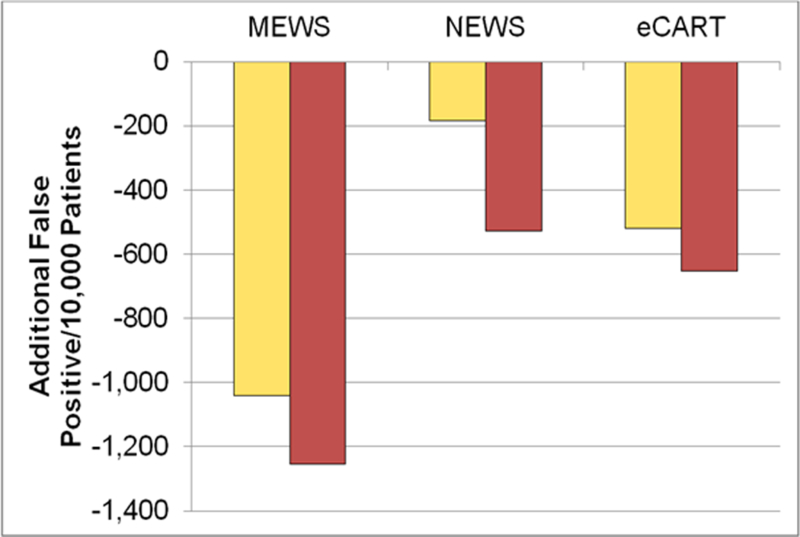
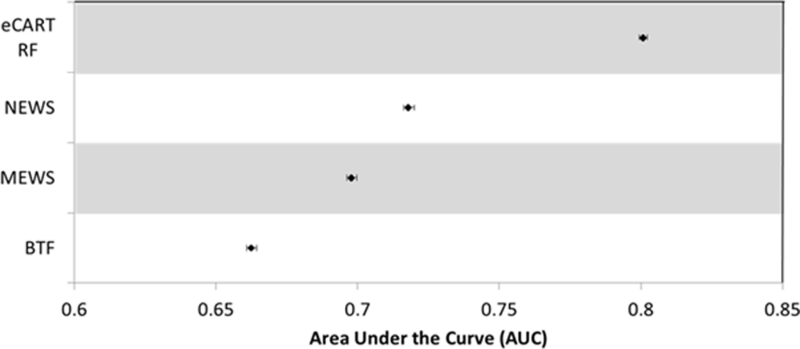
Main outcome measures: Cardiac arrest, ICU transfer or death within 24h of a score RESULTS: Overall accuracy was highest for eCART, with an AUC of 0.801 (95% CI 0.799-0.802), followed by NEWS, MEWS and BTF respectively (0.718 [0.716-0.720]; 0.698 [0.696-0.700]; 0.663 [0.661-0.664]). BTF criteria had a high risk (Red Zone) specificity of 95.0% and a moderate risk (Yellow Zone) specificity of 27.5%, which corresponded to MEWS thresholds of >=4 and >=2, NEWS thresholds of >=5 and >=2, and eCART thresholds of >=12 and >=4, respectively. At those thresholds, eCART caught 22 more adverse events per 10,000 patients than BTF using the moderate risk criteria and 13 more using high risk criteria, while MEWS and NEWS identified the same or fewer.
Conclusion(s): An electronically generated eCART score was more accurate than commonly used paper based observation tools for predicting the composite outcome of in-hospital cardiac arrest, ICU transfer and death within 24h of observation. The outcomes of this analysis lend weight for a move towards an algorithm based electronic risk identification tool for deteriorating patients to ensure earlier detection and prevent adverse events in the hospital.
Keywords: Decision support; Deteriorating patients; Early warning scores; MEWS; NEWS; Rapid response systems.
Copyright © 2017 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
In search of the 'best' rapid response early warning system - The journey has just begun.Resuscitation. 2018 Feb;123:A1-A2. doi: 10.1016/j.resuscitation.2017.12.005. Epub 2017 Dec 11. Resuscitation. 2018. PMID: 29242056 No abstract available.
Similar articles
-
Predicting clinical deterioration with Q-ADDS compared to NEWS, Between the Flags, and eCART track and trigger tools.Resuscitation. 2020 Aug;153:28-34. doi: 10.1016/j.resuscitation.2020.05.027. Epub 2020 Jun 3. Resuscitation. 2020. PMID: 32504769 Free PMC article.
-
Validating the Electronic Cardiac Arrest Risk Triage (eCART) Score for Risk Stratification of Surgical Inpatients in the Postoperative Setting: Retrospective Cohort Study.Ann Surg. 2019 Jun;269(6):1059-1063. doi: 10.1097/SLA.0000000000002665. Ann Surg. 2019. PMID: 31082902 Free PMC article.
-
Comparison of early warning scores for predicting clinical deterioration and infection in obstetric patients.BMC Pregnancy Childbirth. 2022 Apr 6;22(1):295. doi: 10.1186/s12884-022-04631-0. BMC Pregnancy Childbirth. 2022. PMID: 35387624 Free PMC article.
-
The use of early warning system scores in prehospital and emergency department settings to predict clinical deterioration: A systematic review and meta-analysis.PLoS One. 2022 Mar 17;17(3):e0265559. doi: 10.1371/journal.pone.0265559. eCollection 2022. PLoS One. 2022. PMID: 35298560 Free PMC article.
-
A review of early warning systems for prompt detection of patients at risk for clinical decline.J Trauma Acute Care Surg. 2019 Jul;87(1S Suppl 1):S67-S73. doi: 10.1097/TA.0000000000002197. J Trauma Acute Care Surg. 2019. PMID: 31246909 Review.
Cited by
-
Fast Healthcare Interoperability Resources for Inpatient Deterioration Detection With Time-Series Vital Signs: Design and Implementation Study.JMIR Med Inform. 2022 Oct 13;10(10):e42429. doi: 10.2196/42429. JMIR Med Inform. 2022. PMID: 36227636 Free PMC article.
-
Assessing the Usability of a Novel Wearable Remote Patient Monitoring Device for the Early Detection of In-Hospital Patient Deterioration: Observational Study.JMIR Form Res. 2022 Jun 9;6(6):e36066. doi: 10.2196/36066. JMIR Form Res. 2022. PMID: 35679119 Free PMC article.
-
Effect of an Electronic Medical Record-Based Screening System on a Rapid Response System: 8-Years' Experience of a Single Center Cohort.J Clin Med. 2020 Feb 1;9(2):383. doi: 10.3390/jcm9020383. J Clin Med. 2020. PMID: 32024053 Free PMC article.
-
Predicting Patient Deterioration: A Review of Tools in the Digital Hospital Setting.J Med Internet Res. 2021 Sep 30;23(9):e28209. doi: 10.2196/28209. J Med Internet Res. 2021. PMID: 34591017 Free PMC article. Review.
-
Development and validation of early warning score system: A systematic literature review.J Biomed Inform. 2020 May;105:103410. doi: 10.1016/j.jbi.2020.103410. Epub 2020 Apr 8. J Biomed Inform. 2020. PMID: 32278089 Free PMC article.
References
-
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalised patients: results of the Harvard Medical Practice Study I. N Engl J Med 1991; 324: 370–77. - PubMed
-
- Wilson RM, Runciman WB, Gibberd RW, et al. The quality in Australian Health Care Study. Med J Aust 1995; 163: 458–76. - PubMed
-
- Davis P, Lay-Yee R, Briant R, et al. Adverse events in New Zealand public hospitals I: occurrence and impact N Z Med J 2002; 115: 271. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
