

Analysis of Fusobacterium persistence and antibiotic response in colorectal cancer
- PMID: 29170280
- PMCID: PMC5823247
- DOI: 10.1126/science.aal5240
Analysis of Fusobacterium persistence and antibiotic response in colorectal cancer
Abstract
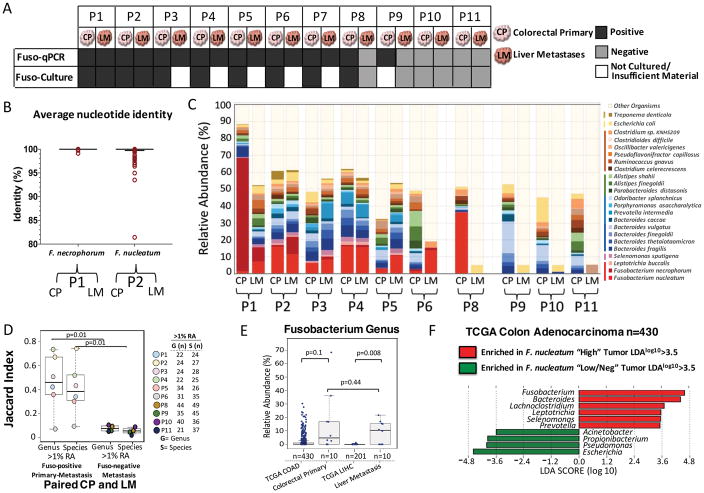
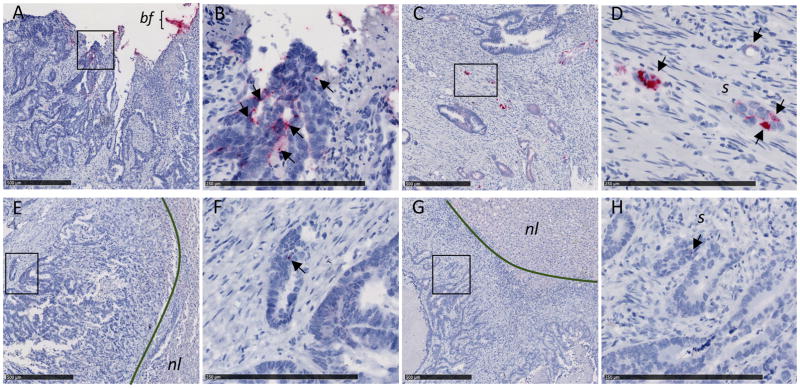
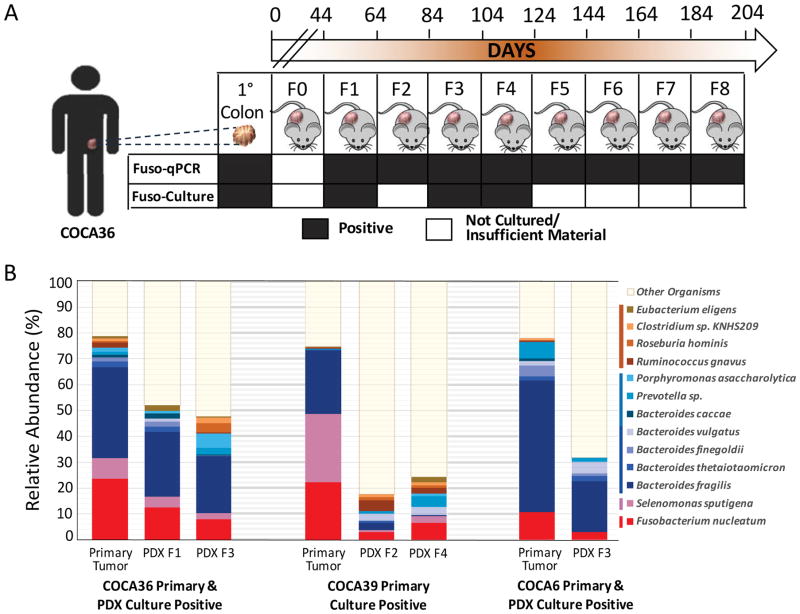
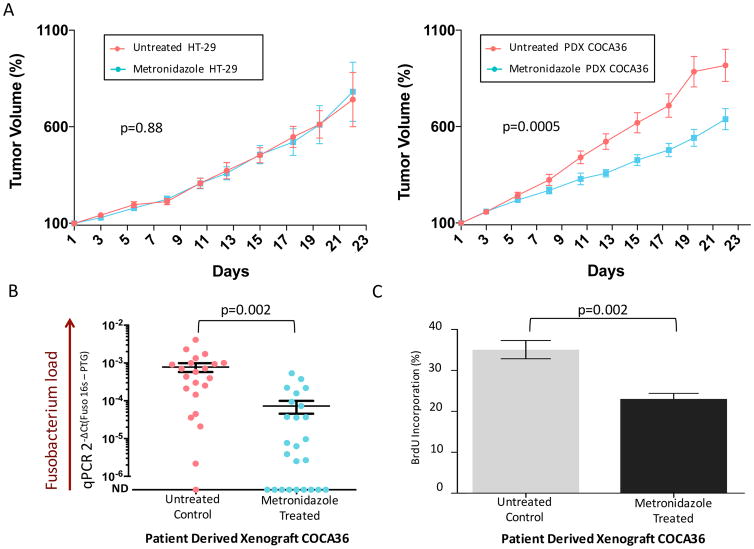
Colorectal cancers comprise a complex mixture of malignant cells, nontransformed cells, and microorganisms. Fusobacterium nucleatum is among the most prevalent bacterial species in colorectal cancer tissues. Here we show that colonization of human colorectal cancers with Fusobacterium and its associated microbiome-including Bacteroides, Selenomonas, and Prevotella species-is maintained in distal metastases, demonstrating microbiome stability between paired primary and metastatic tumors. In situ hybridization analysis revealed that Fusobacterium is predominantly associated with cancer cells in the metastatic lesions. Mouse xenografts of human primary colorectal adenocarcinomas were found to retain viable Fusobacterium and its associated microbiome through successive passages. Treatment of mice bearing a colon cancer xenograft with the antibiotic metronidazole reduced Fusobacterium load, cancer cell proliferation, and overall tumor growth. These observations argue for further investigation of antimicrobial interventions as a potential treatment for patients with Fusobacterium-associated colorectal cancer.
Copyright © 2017 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Comment in
-
Microbiome: Fusobacterium persistence in colorectal cancer.Nat Rev Microbiol. 2017 Dec 8;16(1):2. doi: 10.1038/nrmicro.2017.164. Nat Rev Microbiol. 2017. PMID: 29217844 No abstract available.
-
Colorectal cancer: Hand-in-hand - colorectal cancer metastasizes with microorganisms.Nat Rev Gastroenterol Hepatol. 2018 Mar;15(3):133-134. doi: 10.1038/nrgastro.2017.186. Epub 2018 Jan 17. Nat Rev Gastroenterol Hepatol. 2018. PMID: 29339812 No abstract available.
-
Integrating microbiomics in cancer management.Nat Rev Cancer. 2021 Nov;21(11):684-685. doi: 10.1038/s41568-021-00392-8. Nat Rev Cancer. 2021. PMID: 34316056 No abstract available.
References
-
- Arthur JC, Perez-Chanona E, Mühlbauer M, Tomkovich S, Uronis JM, Fan TJ, Campbell BJ, Abujamel T, Dogan B, Rogers AB, Rhodes JM, Stintzi A, Simpson KW, Hansen JJ, Keku TO, Fodor AA, Jobin C. Intestinal inflammation targets cancer-inducing activity of the microbiota. Science. 2012;338:120–123. doi: 10.1126/science.1224820. - DOI - PMC - PubMed
-
- Wu S, Rhee KJ, Albesiano E, Rabizadeh S, Wu X, Yen HR, Huso DL, Brancati FL, Wick E, McAllister F, Housseau F, Pardoll DM, Sears CL. A human colonic commensal promotes colon tumorigenesis via activation of T helper type 17 T cell responses. Nat Med. 2009;15:1016–1022. doi: 10.1038/nm.2015. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
