

Increasing motor neuron excitability to treat weakness in sepsis
- PMID: 29171917
- PMCID: PMC5739976
- DOI: 10.1002/ana.25105
Increasing motor neuron excitability to treat weakness in sepsis
Abstract
Objective: Weakness induced by critical illness (intensive care unit acquired weakness) is a major cause of disability in patients and is currently untreatable. We recently identified a defect in repetitive firing of lower motor neurons as a novel contributor to intensive care unit acquired weakness. To develop therapy for intensive care unit acquired weakness, it was necessary to determine the mechanism underlying the defect in repetitive firing.
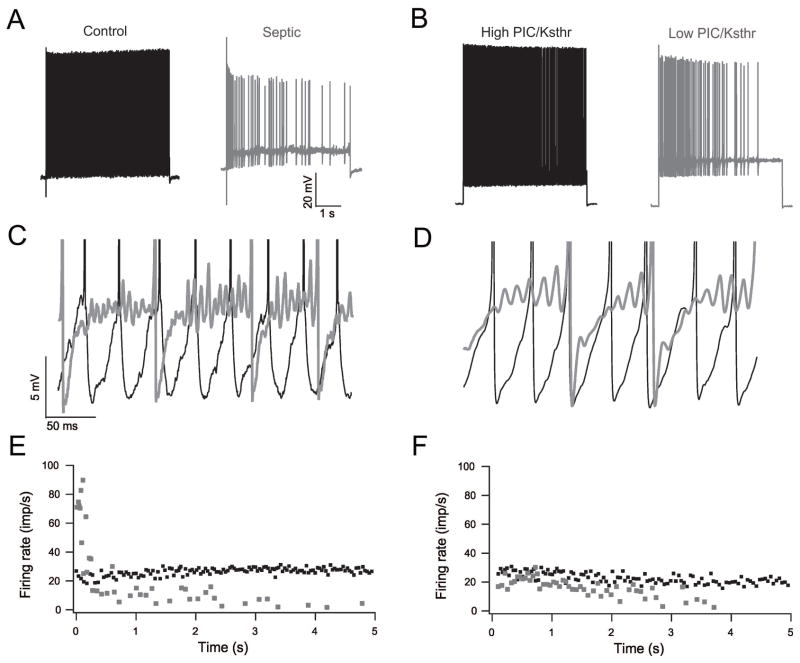
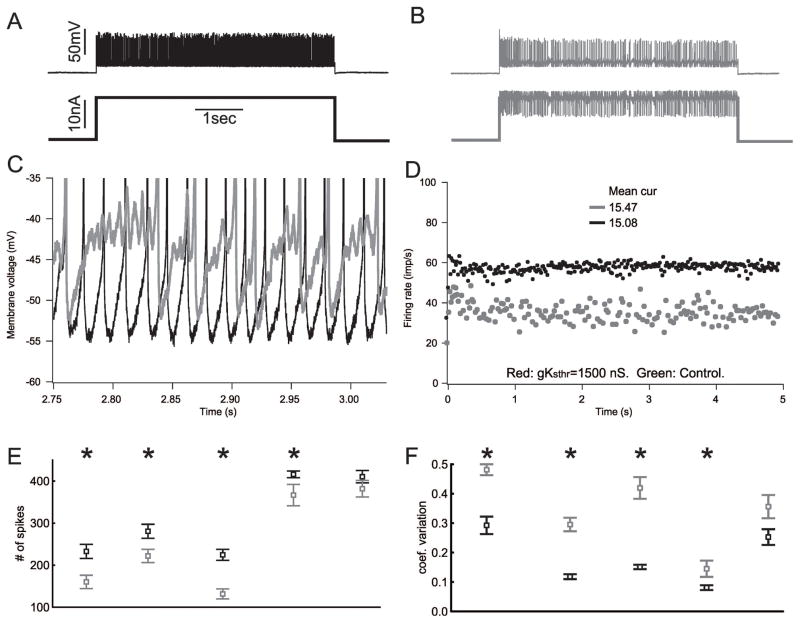
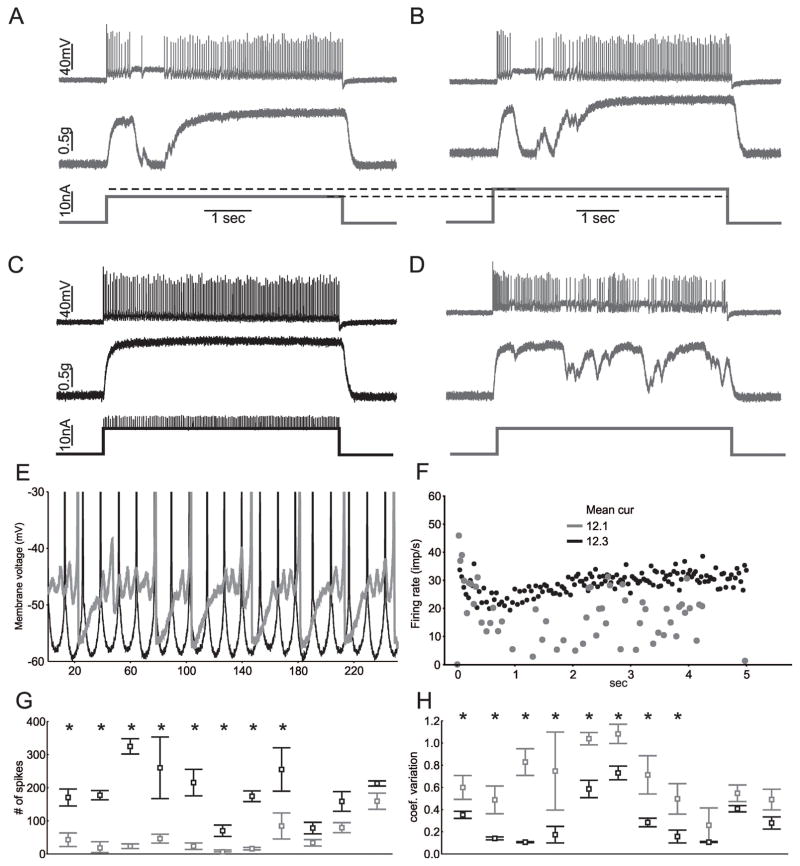
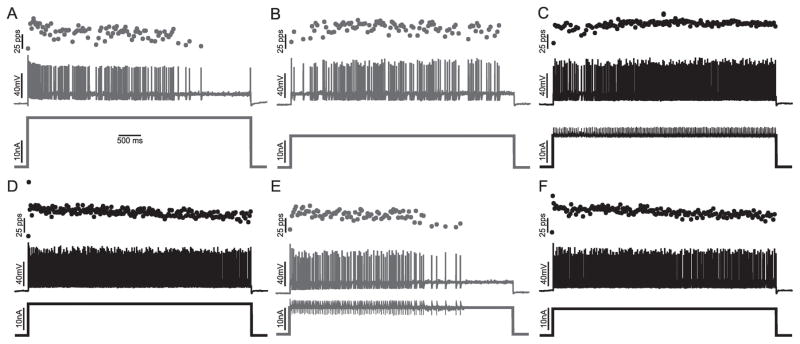
Methods: Both computer simulation and in vivo dynamic voltage clamp of spinal motor neurons in septic rats were employed to explore potential mechanisms underlying defective repetitive firing.
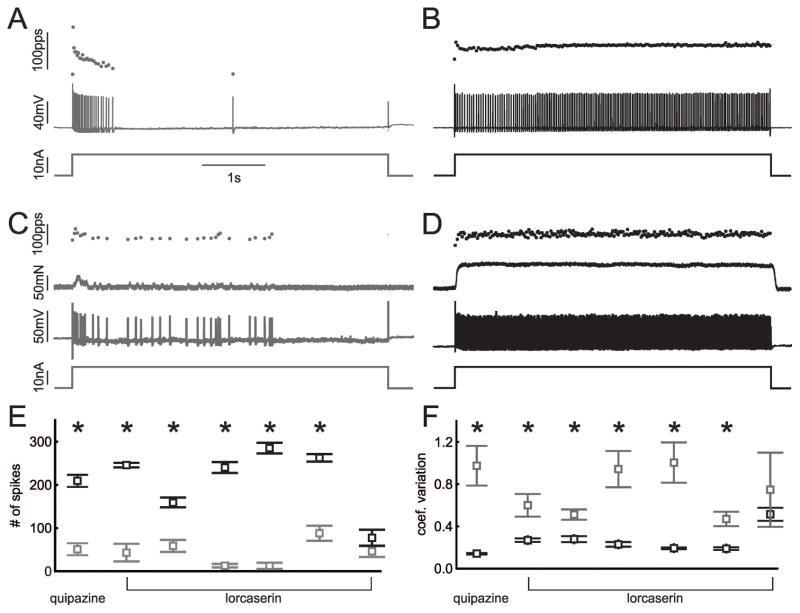
Results: Our results suggest alteration in subthreshold voltage-activated currents might be the mechanism underlying defective repetitive firing. It has been shown previously that pharmacologic activation of serotonin receptors on motor neurons increases motor neuron excitability, in part by enhancing subthreshold voltage-activated inward currents. Administration of a U.S. Food and Drug Administration-approved serotonin agonist (lorcaserin) to septic rats greatly improved repetitive firing and motor unit force generation.
Interpretation: Our findings suggest activation of serotonin receptors with lorcaserin may provide the first ever therapy for intensive care unit acquired weakness in patients. Ann Neurol 2017;82:961-971.
© 2017 American Neurological Association.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
Similar articles
-
Imbalanced Subthreshold Currents Following Sepsis and Chemotherapy: A Shared Mechanism Offering a New Therapeutic Target?Neuroscientist. 2022 Apr;28(2):103-120. doi: 10.1177/1073858420981866. Epub 2020 Dec 21. Neuroscientist. 2022. PMID: 33345706 Free PMC article.
-
Reduced motor neuron excitability is an important contributor to weakness in a rat model of sepsis.Exp Neurol. 2016 Aug;282:1-8. doi: 10.1016/j.expneurol.2016.04.020. Epub 2016 Apr 24. Exp Neurol. 2016. PMID: 27118372 Free PMC article.
-
Reduced motoneuron excitability in a rat model of sepsis.J Neurophysiol. 2013 Apr;109(7):1775-81. doi: 10.1152/jn.00936.2012. Epub 2013 Jan 9. J Neurophysiol. 2013. PMID: 23303860 Free PMC article.
-
Persistent inward currents in motoneuron dendrites: implications for motor output.Muscle Nerve. 2005 Feb;31(2):135-56. doi: 10.1002/mus.20261. Muscle Nerve. 2005. PMID: 15736297 Review.
-
Does the frequency content of the surface mechanomyographic signal reflect motor unit firing rates? A brief review.J Electromyogr Kinesiol. 2007 Feb;17(1):1-13. doi: 10.1016/j.jelekin.2005.12.002. Epub 2006 Feb 23. J Electromyogr Kinesiol. 2007. PMID: 16497517 Review.
Cited by
-
Reduced Neural Excitability and Activation Contribute to Clinically Meaningful Weakness in Older Adults.J Gerontol A Biol Sci Med Sci. 2021 Mar 31;76(4):692-702. doi: 10.1093/gerona/glaa157. J Gerontol A Biol Sci Med Sci. 2021. PMID: 32588058 Free PMC article.
-
Structural Preservation Does Not Ensure Function at Sensory Ia-Motoneuron Synapses following Peripheral Nerve Injury and Repair.J Neurosci. 2023 Jun 14;43(24):4390-4404. doi: 10.1523/JNEUROSCI.0103-23.2023. Epub 2023 May 1. J Neurosci. 2023. PMID: 37127364 Free PMC article.
-
Central Role of Subthreshold Currents in Myotonia.Ann Neurol. 2020 Feb;87(2):175-183. doi: 10.1002/ana.25646. Epub 2019 Nov 27. Ann Neurol. 2020. PMID: 31725924 Free PMC article. Review.
-
The mechanism underlying transient weakness in myotonia congenita.Elife. 2021 Apr 27;10:e65691. doi: 10.7554/eLife.65691. Elife. 2021. PMID: 33904400 Free PMC article.
-
Imbalanced Subthreshold Currents Following Sepsis and Chemotherapy: A Shared Mechanism Offering a New Therapeutic Target?Neuroscientist. 2022 Apr;28(2):103-120. doi: 10.1177/1073858420981866. Epub 2020 Dec 21. Neuroscientist. 2022. PMID: 33345706 Free PMC article.
References
-
- Stevens RD, Marshall SA, Cornblath DR, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Critical Care Medicine. 2009;37:S299–308. - PubMed
-
- Latronico N, Bolton CF. Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis. Lancet Neurol. 2011;10:931–941. - PubMed
-
- van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
