

Multi-Drug-Resistant Gram-Negative Infections in Deployment-Related Trauma Patients
- PMID: 29173084
- PMCID: PMC5393413
- DOI: 10.1089/sur.2017.002
Multi-Drug-Resistant Gram-Negative Infections in Deployment-Related Trauma Patients
Abstract
Background: The contribution of multi-drug-resistant gram-negative bacilli infections (MDRGN-I) in patients with trauma is not well described. We present characteristics of MDRGN-Is among military personnel with deployment-related trauma (2009-2014).
Patients and methods: Data from the Trauma Infectious Disease Outcomes Study were assessed for infectious outcomes and microbial recovery. Infections were classified using standardized definitions. Gram-negative bacilli were defined as multi-drug-resistant if they showed resistance to ≥3 antibiotic classes or were producers of extended-spectrum β-lactamase or carbapenemases.
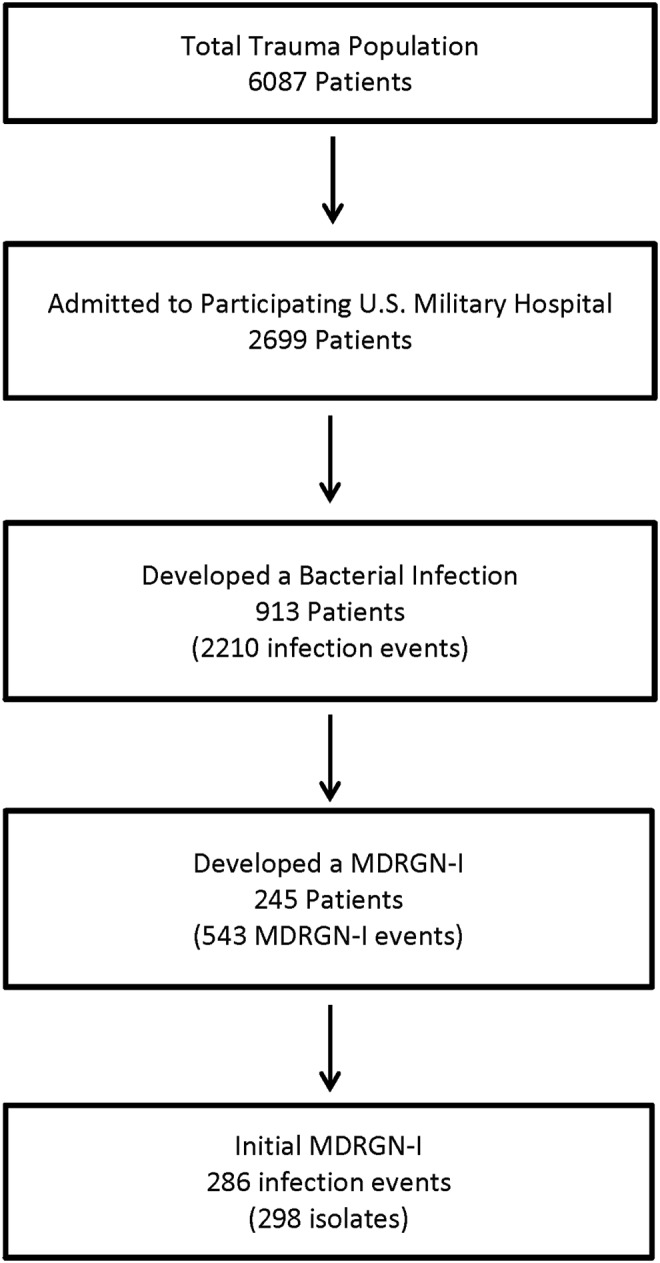
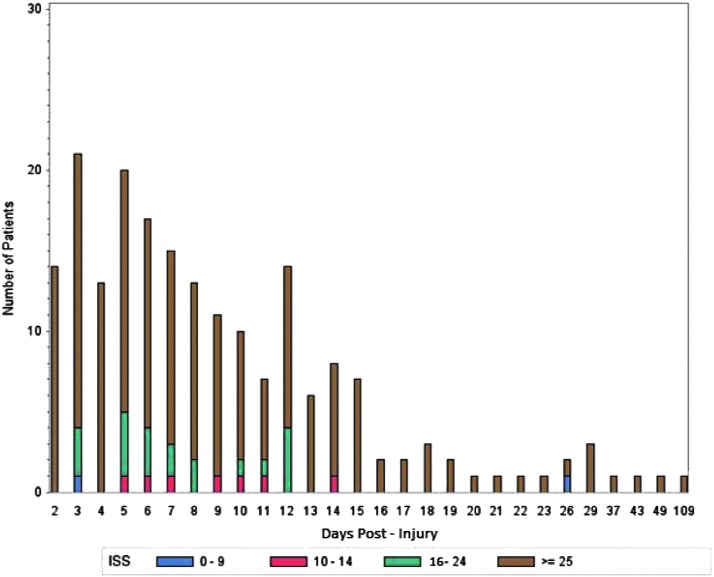
Results: Among 2,699 patients admitted to participating U.S. hospitals, 913 (33.8%) experienced ≥1 infection event, of which 245 (26.8%) had a MDRGN-I. There were 543 MDRGN-I events (24.6% of unique 2,210 infections) with Escherichia coli (48.3%), Acinetobacter spp. (38.6%), and Klebsiella pneumoniae (8.4%) as the most common MDRGN isolates. Incidence of MDRGN-I was 9.1% (95% confidence interval [CI]: 8.0-10.2). Median time to MDRGN-I event was seven days with 75% occurring within 13 days post-trauma. Patients with MDRGN-Is had a greater proportion of blast injuries (84.1% vs. 62.5%; p < 0.0001), traumatic amputations (57.5% vs. 16.3%; p < 0.0001), and higher injury severity (82.0% had injury severity score ≥25 vs. 33.7%; p < 0.0001) compared with patients with either no infections or non-MDRGN-Is. Furthermore, MDRGN-I patients were more frequently admitted to the intensive care unit (90.5% vs. 48.5%; p < 0.0001), colonized with a MDRGN before infection (58.0% vs. 14.7%; p < 0.0001), and required mechanical ventilation (78.0% vs. 28.8% p < 0.0001). Antibiotic exposure before the MDRGN-I event was significantly higher across antibiotic classes except first generation cephalosporins and tetracyclines, which were very commonly used with all patients. Regarding outcomes, patients with MDRGN-Is had a longer length of hospitalization than the comparator group (53 vs. 18 days; p < 0.0001).
Conclusions: We found a high rate of MDRGN-I in our population characterized by longer hospitalization and greater injury severity. These findings inform treatment and infection control decisions in the trauma patient population.
Keywords: gram-negative bacilli; multi-drug–resistant organisms; trauma-related infections.
Conflict of interest statement
No competing financial interests exist.
The views expressed are those of the authors and does not necessarily reflect the official views of the Uniformed Services University of the Health Sciences, Henry M. Jackson Foundation for the Advancement of Military Medicine, National Institutes of Health or the Department of Health and Human Services, Walter Reed National Military Medical Center, Landstuhl Regional Medical Center, Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of Defense or the Departments of the Army, Navy or Air Force. Mention of trade names, commercial products, or organization does not imply endorsement by the U.S. Government.'
Figures



References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: www.cdc.gov/drugresistance/threat-report-2013 2013. (Last accessed December12, 2016)
-
- The President's Council of Advisors on Science and Technology. Report to the President on Combatting Antibiotic Resistance. www.whitehouse.gov/sites/default/files/microsites/ostp/PCAST/pcast_carb_... 2014. (Last accessed December12, 2016)
-
- Nathan C, Cars O. Antibiotic resistance—problems, progress, and prospects. N Engl J Med 2014;371:1761–1763 - PubMed
-
- Dortch MJ, Fleming SB, Kauffmann RM, et al. Infection reduction strategies including antibiotic stewardship protocols in surgical and trauma intensive care units are associated with reduced resistant gram-negative healthcare-associated infections. Surg Infect (Larchmt) 2011;12:15–25 - PubMed
-
- Jean SS, Ko WC, Xie Y, et al. Clinical characteristics of patients with community-acquired complicated intra-abdominal infections: A prospective, multicentre, observational study. Int J Antimicrob Agents 2014;44:222–228 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
