

Targeted Family Intervention for Complex Cases of Pediatric Obsessive-Compulsive Disorder: A Randomized Controlled Trial
- PMID: 29173737
- PMCID: PMC5875916
- DOI: 10.1016/j.jaac.2017.10.008
Targeted Family Intervention for Complex Cases of Pediatric Obsessive-Compulsive Disorder: A Randomized Controlled Trial
Abstract
Objective: Although evidence-based treatments for pediatric obsessive-compulsive disorder (OCD) exist, many youth fail to respond, and interventions tailored to the needs of specific subsets of patients are lacking. This study examines the efficacy of a family intervention module designed for cases of OCD complicated by poor family functioning.
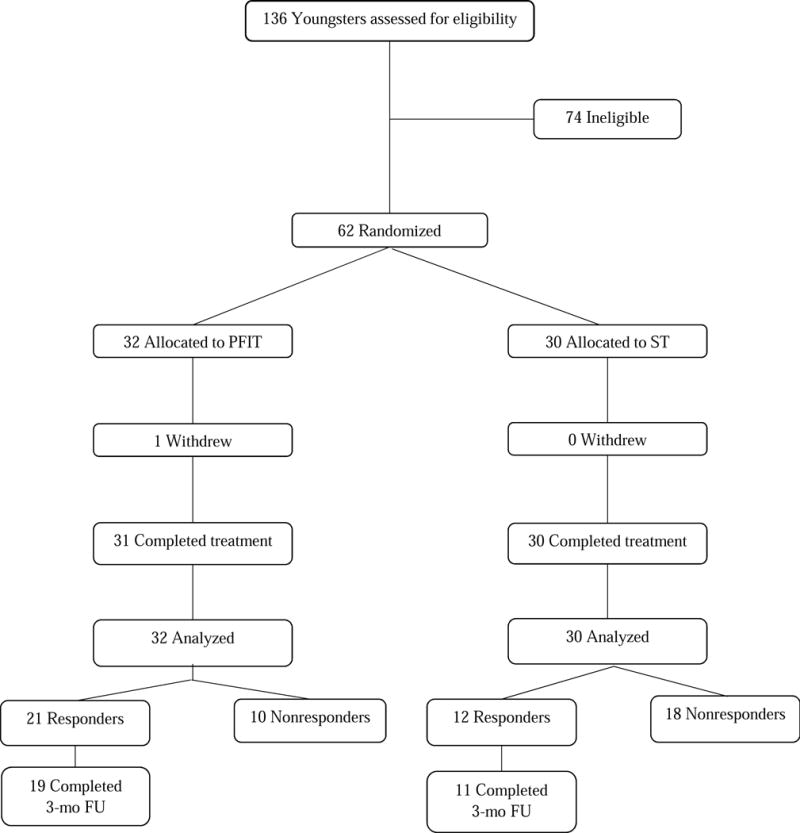
Method: Participants were 62 youngsters aged 8 to 17 years (mean age = 12.71 years; 57% male; 65% white) with a primary diagnosis of OCD and at least 2 indicators of poor family functioning. They were randomized to receive 12 sessions of individual child cognitive-behavioral therapy (CBT) plus weekly parent psychoeducation and session review (standard treatment [ST]) or the same 12 child sessions plus 6 sessions of family therapy aimed at improving OCD-related emotion regulation and problem solving (positive family interaction therapy [PFIT]). Blinded raters evaluated outcomes and tracked responders to 3-month follow-up.
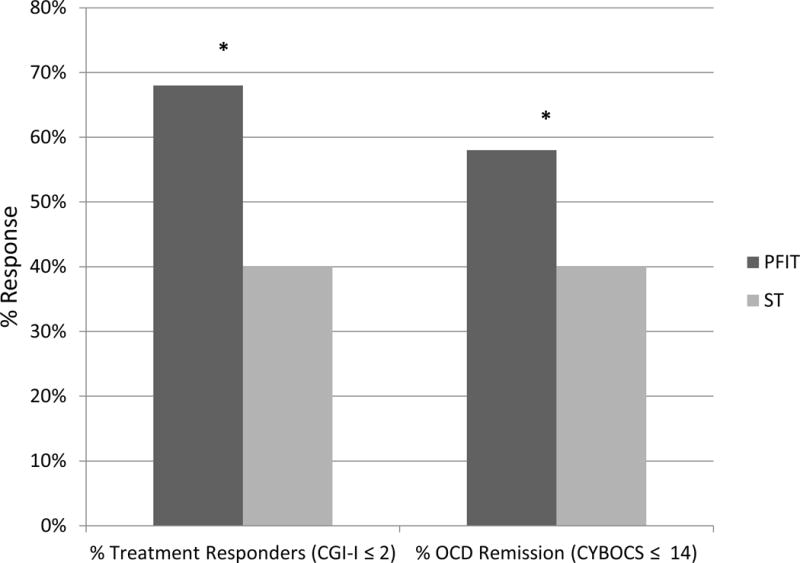
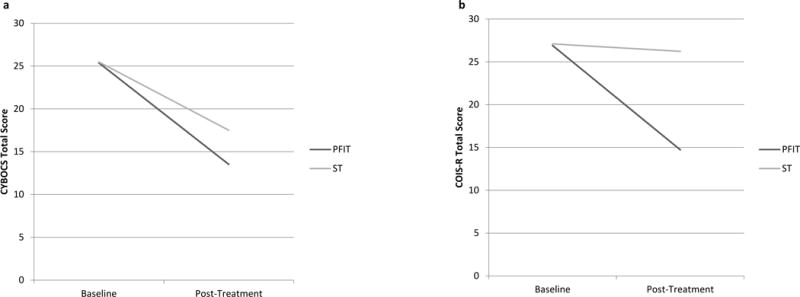
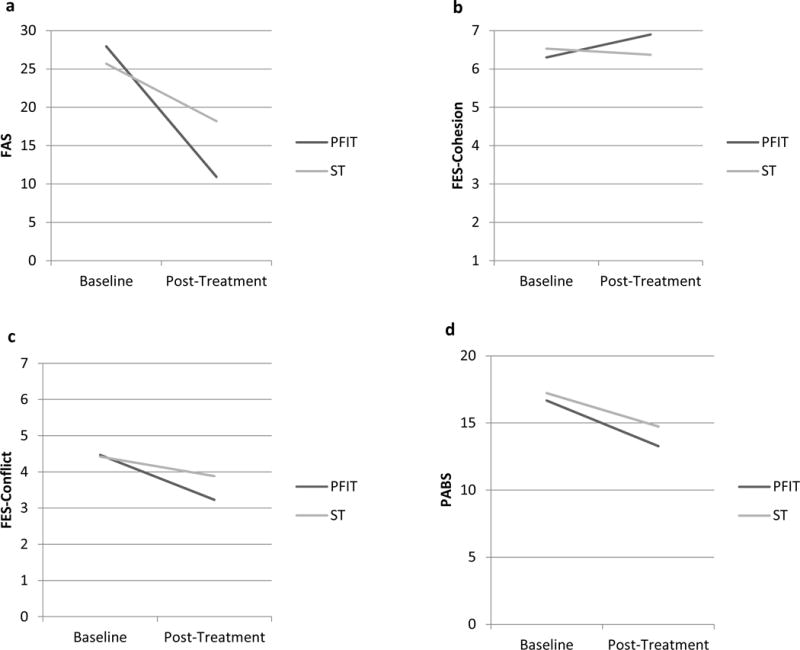
Results: Compared to ST, PFIT demonstrated better overall response rates on the Clinician Global Impression-Improvement scale (CGI-I; 68% versus 40%, p = .03, φ = 0.28) and rates of remission (58% PFIT versus 27% ST, p = .01, φ = 0.32). PFIT also produced significantly greater reductions in functional impairment, symptom accommodation, and family conflict, and improvements in family cohesion. As expected, these shifts in family functioning constitute an important treatment mechanism, with changes in accommodation mediating treatment response.
Conclusion: PFIT is efficacious for reducing OCD symptom severity and impairment and for improving family functioning. Findings are discussed in terms of personalized medicine and mechanisms of change in pediatric OCD treatment. Clinical trial registration information-Family Focused Treatment of Pediatric Obsessive Compulsive Disorder; http://clinicaltrials.gov/; NCT01409642.
Keywords: CBT; exposure; family treatment; pediatric OCD.
Copyright © 2017 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Piacentini J, Peris TS, Bergman RL, Chang S, Jaffer M. Functional impairment in childhood ocd: Development and psychometrics properties of the child obsessive-compulsive impact scale-revised (COIS-R) J Clin Child Adolesc Psychol. 2007;36(4):645–53. - PubMed
-
- Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry. 1998;55:56–64. - PubMed
-
- Geller DA, Marsch JS, Walter HJ, et al. Practice parameter for the assessment and treatment of children and adolescents with obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry. 2012;51(1):98–113. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
