

Incidence of drug-induced torsades de pointes with intravenous amiodarone
- PMID: 29174246
- PMCID: PMC5717288
- DOI: 10.1016/j.ihj.2017.05.024
Incidence of drug-induced torsades de pointes with intravenous amiodarone
Abstract
Aim: To define the incidence, presentation, and outcomes of drug-induced Torsades de Pointes (TdP) with intravenous (IV) amiodarone.
Methods: From January 2014 to August 2016 a total of 268 patients received IV amiodarone, 142 for ventricular tachycardia, 104 for atrial flutter/fibrillation, and 22 for incessant atrial tachycardia. A uniform dosing of amiodarone to yield 1gm/day was used in all patients.
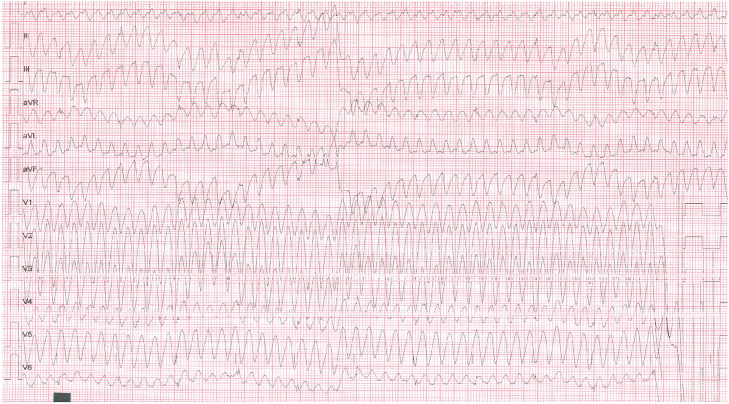
Results: Four of the 268 patients (M:F 1:3) with mean age of 51.25+9.17years developed pause dependent TdP degenerating to VF, after a mean dose of 690+176.63mg, infused over 12+5.88h. The QTc that was 505+9.02ms at the time of TdP normalized to 433.75+6.13ms 48-72h after stopping amiodarone. There was no immediate or late mortality, and patients are well at 5-10 months of follow-up. None of the patients tested positive for LQTS genes.
Conclusion: The incidence of drug-induced TdP with IV amiodarone is about 1.5%. Risk factors include female sex, left ventricular dysfunction, electrolyte abnormalities, baseline prolonged QTc, concomitant beta-blocker, and digoxin therapy. Amiodarone induced TdP has favorable prognosis if recognized and treated promptly, and these patients should not receive amiodarone by any route in future.
Keywords: Acquired LQT; Amiodarone; Proarrhythmia; Torsades de pointes.
Copyright © 2017 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
Figures


Similar articles
-
[Torsades de pointes ventricular tachycardia induced by intravenous amiodarone].Orv Hetil. 2003 Feb 2;144(5):241-7. Orv Hetil. 2003. PMID: 12647553 Review. Hungarian.
-
Amiodarone-induced torsade de pointes in a patient with wolff-Parkinson-White syndrome.Hellenic J Cardiol. 2009 May-Jun;50(3):224-6. Hellenic J Cardiol. 2009. PMID: 19465366
-
Early proarrhythmia during intravenous amiodarone treatment.Pacing Clin Electrophysiol. 1999 Jun;22(6 Pt 1):968-70. doi: 10.1111/j.1540-8159.1999.tb06827.x. Pacing Clin Electrophysiol. 1999. PMID: 10392400
-
Further evidence of inherited long QT syndrome gene mutations in antiarrhythmic drug-associated torsades de pointes.Heart Rhythm. 2007 May;4(5):603-7. doi: 10.1016/j.hrthm.2007.01.019. Epub 2007 Jan 18. Heart Rhythm. 2007. PMID: 17467628
-
QTc prolongation and torsades de pointes due to a coadministration of fluoxetine and amiodarone in a patient with implantable cardioverter-defibrillator: Case report and review of the literature.Medicine (Baltimore). 2017 Dec;96(49):e9071. doi: 10.1097/MD.0000000000009071. Medicine (Baltimore). 2017. PMID: 29245320 Free PMC article. Review.
Cited by
-
Suppression of amiodarone-induced torsade de pointes by landiolol in a patient with atrial fibrillation-mediated cardiomyopathy.Ann Noninvasive Electrocardiol. 2021 Nov;26(6):e12842. doi: 10.1111/anec.12842. Epub 2021 Mar 23. Ann Noninvasive Electrocardiol. 2021. PMID: 33755267 Free PMC article.
-
Complete Heart Block Induced Torsades de Pointes.Cureus. 2024 Feb 28;16(2):e55169. doi: 10.7759/cureus.55169. eCollection 2024 Feb. Cureus. 2024. PMID: 38558635 Free PMC article.
-
Update of Takotsubo cardiomyopathy: Present experience and outlook for the future.Int J Cardiol Heart Vasc. 2022 Mar 7;39:100990. doi: 10.1016/j.ijcha.2022.100990. eCollection 2022 Apr. Int J Cardiol Heart Vasc. 2022. PMID: 35281752 Free PMC article. Review.
-
Amiodarone in junctional ectopic tachycardia: A word of caution!J Anaesthesiol Clin Pharmacol. 2021 Apr-Jun;37(2):302-304. doi: 10.4103/joacp.JOACP_403_19. Epub 2021 Jul 15. J Anaesthesiol Clin Pharmacol. 2021. PMID: 34349389 Free PMC article. No abstract available.
-
Adverse events in different administration routes of amiodarone: a pharmacovigilance study based on the FDA adverse event reporting system.Front Pharmacol. 2025 Jan 27;16:1517616. doi: 10.3389/fphar.2025.1517616. eCollection 2025. Front Pharmacol. 2025. PMID: 39931689 Free PMC article.
References
-
- Connolly S.J. Evidence based analysis of amiodarone efficacy and safety. Circulation. 1999;100:2025–2034. - PubMed
-
- Scheinman M.M., Levine J.H., Cannom D.S. Dose-ranging study of intravenous amiodarone in patients with life-threatening ventricular tachyarrhythmias. Circulation. 1995;92(December (11)):3264–3272. - PubMed
-
- Clemo H.F., Wood M.A., Gilligan D.M., Ellenbogen K.A. Intravenous amiodarone for acute heart with atrial tachyarrhythmias. Am J Cardiol. 1998;81(97):594–598. - PubMed
-
- Kirchhof P., Benussi S., Kotecha D. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(October (38)):2893–2962. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
