

Predictive modeling for determination of microscopic residual disease at primary cytoreduction: An NRG Oncology/Gynecologic Oncology Group 182 Study
- PMID: 29174555
- PMCID: PMC5962447
- DOI: 10.1016/j.ygyno.2017.10.011
Predictive modeling for determination of microscopic residual disease at primary cytoreduction: An NRG Oncology/Gynecologic Oncology Group 182 Study
Abstract
Objective: Microscopic residual disease following complete cytoreduction (R0) is associated with a significant survival benefit for patients with advanced epithelial ovarian cancer (EOC). Our objective was to develop a prediction model for R0 to support surgeons in their clinical care decisions.
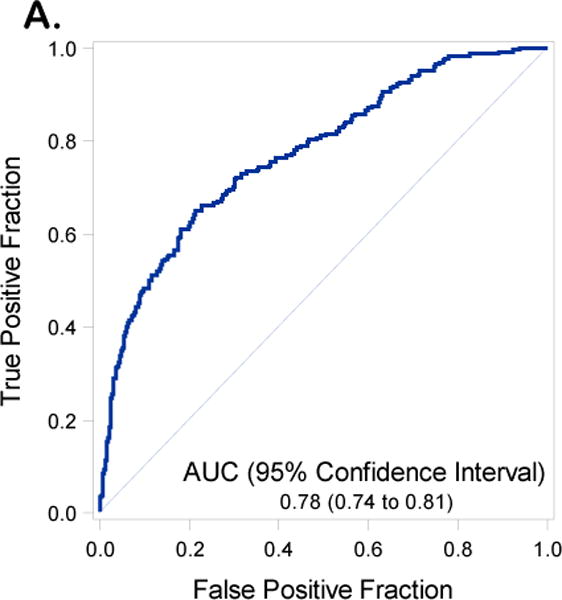
Methods: Demographic, pathologic, surgical, and CA125 data were collected from GOG 182 records. Patients enrolled prior to September 1, 2003 were used for the training model while those enrolled after constituted the validation data set. Univariate analysis was performed to identify significant predictors of R0 and these variables were subsequently analyzed using multivariable regression. The regression model was reduced using backward selection and predictive accuracy was quantified using area under the receiver operating characteristic area under the curve (AUC) in both the training and the validation data sets.
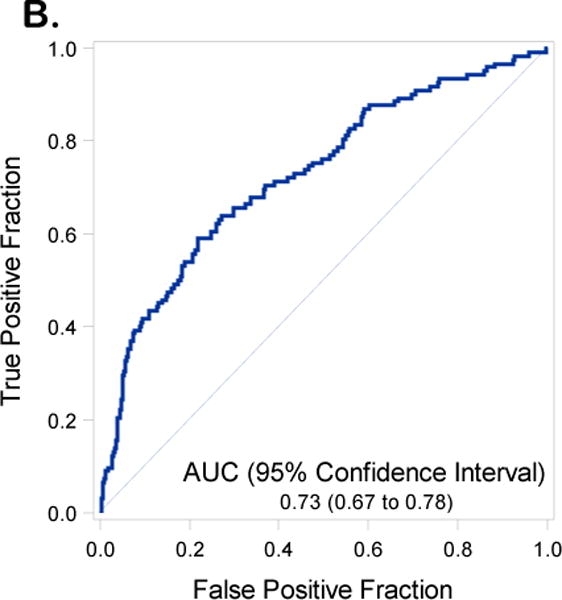
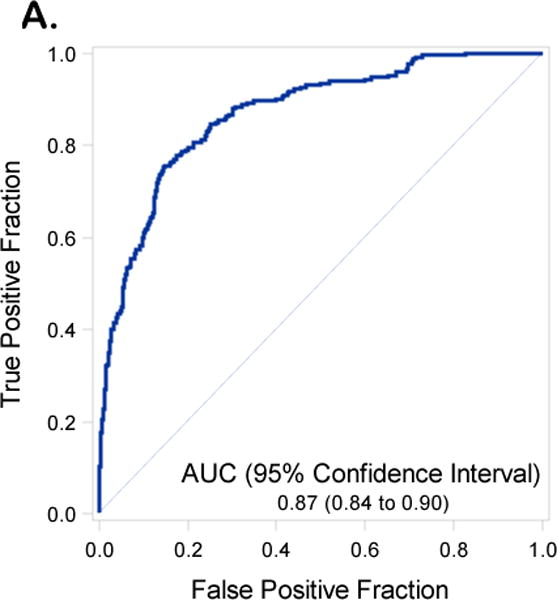
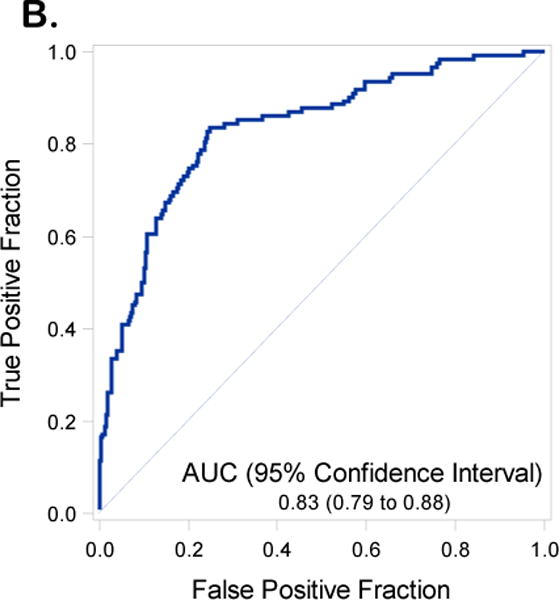
Results: Of the 3882 patients enrolled in GOG 182, 1480 had complete clinical data available for the analysis. The training data set consisted of 1007 patients (234 with R0) while the validation set was comprised of 473 patients (122 with R0). The reduced multivariable regression model demonstrated several variables predictive of R0 at cytoreduction: Disease Score (DS) (p<0.001), stage (p=0.009), CA125 (p<0.001), ascites (p<0.001), and stage-age interaction (p=0.01). Applying the prediction model to the validation data resulted in an AUC of 0.73 (0.67 to 0.78, 95% CI). Inclusion of DS enhanced the model performance to an AUC of 0.83 (0.79 to 0.88, 95% CI).
Conclusions: We developed and validated a prediction model for R0 that offers improved performance over previously reported models for prediction of residual disease. The performance of the prediction model suggests additional factors (i.e. imaging, molecular profiling, etc.) should be explored in the future for a more clinically actionable tool.
Keywords: Microscopic residual; Ovarian cancer.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
All other co-authors have no conflicts of interest to declare.
Figures
References
-
- Chi DS, Eisenhauer EL, Zivanovic O, Sonoda Y, Abu-Rustum NR, Levine DA, et al. Improved progression free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm. Gynecol Oncol. 2009;114:26–31. - PubMed
-
- Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, et al. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol. 2006;03:559–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
