

Immunosenescence in persons with spinal cord injury in relation to urinary tract infections -a cross-sectional study
- PMID: 29176992
- PMCID: PMC5688733
- DOI: 10.1186/s12979-017-0103-6
Immunosenescence in persons with spinal cord injury in relation to urinary tract infections -a cross-sectional study
Abstract
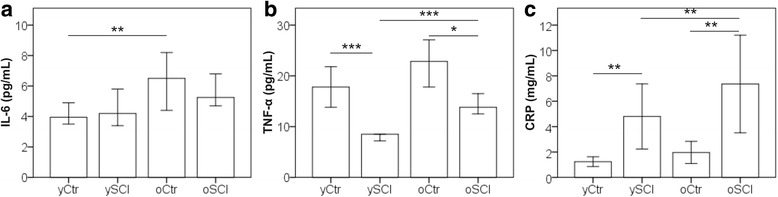
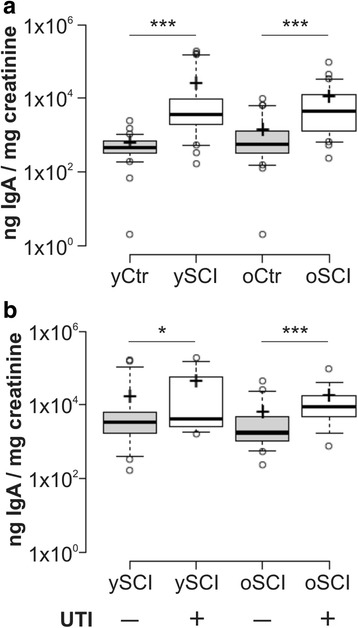
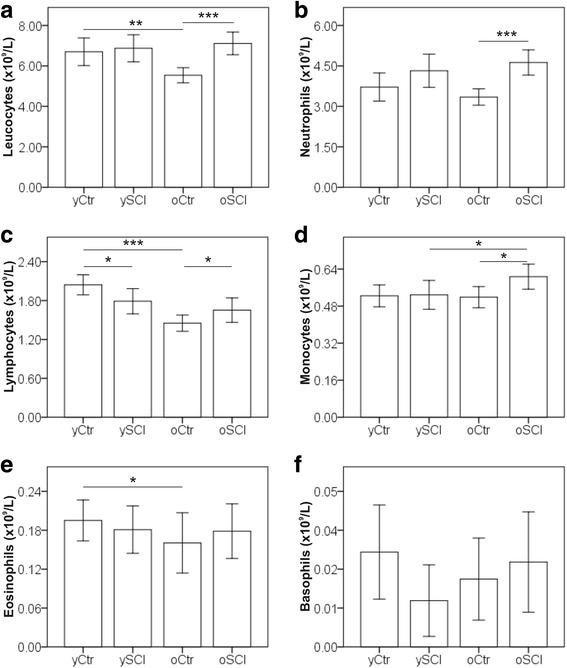
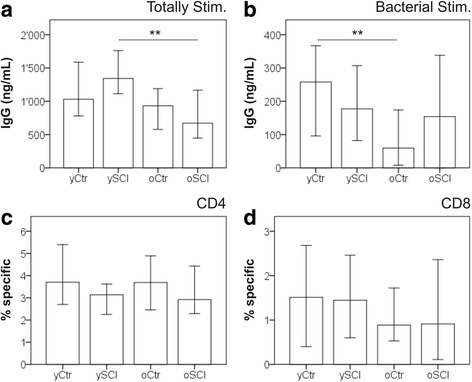
Background: Individuals with a spinal cord injury (SCI), despite specialized rehabilitation and good health care, have a reduced life expectancy. Infectious diseases, such as pneumonias, infected pressure sores and urinary tract infections (UTI) have been identified as the leading causes of mortality. We hypothesise that a premature onset of immune frailty occurs in SCI, possibly caused also by recurrent urinary tract infections.A cross sectional study was performed comparing blood and urine samples between able bodied controls (n = 84) and persons with spinal cord injury (n = 85). The results were grouped according to age (below and above 60 years). Assessed were the abundancies of immune cells, the concentration of soluble biomarkers, the in vitro functioning of lymphocytes as well as phenotypic exhaustion of T-cells in blood and urine. Further, the leucocyte telomere length and the cytomegalovirus (CMV) serological status were compared between the groups.
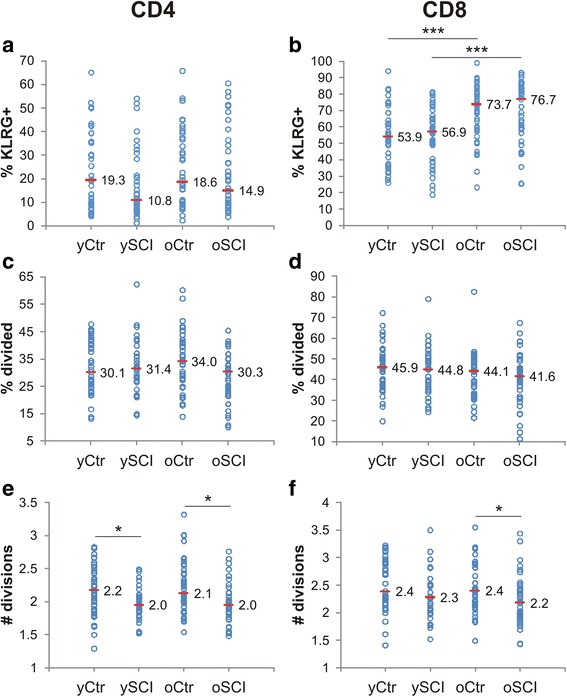
Results: We observed in people with SCI lower proportions of naïve T-cells, more memory T-cells, reduced T-cell proliferation and higher CMV prevalence compared to age-matched controls. SCI participants older than 60 years had a higher prevalence of UTI compared with SCI persons younger than 60 years.
Conclusion: The immune system of people with SCI shows traits of an increased immunological strain and a premature onset of immune frailty. The role of UTI in the onset of immune frailty remains to be elucidated as we did not see significantly higher abundancies of circulating UTI-bacteria specific T-cell clones in persons with SCI. We assume that any impact of UTI on the immune system might be compartmentalized and locally restricted to the urinary tract.
Keywords: Cytomegalovirus; Immune frailty; Immunosenescence; Memory T-cell; Spinal cord injury; Urinary tract infection.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the “Nordwest- und Zentralschweiz (EKNZ)” ethics committee (reference no. 13084). Written informed consent was obtained from each study participant.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Savic G, DeVivo MJ, Frankel HL, Jamous MA, Soni BM, Charlifue S. Long-term survival after traumatic spinal cord injury: a 70-year British study. Spinal Cord. 2017; - PubMed
-
- Spinal Cord Injury . The National Academies Press. 2005. Progress, promise, and priorities.
-
- National Spinal Cord Injury Statistical Center [https://www.nscisc.uab.edu/]. - PubMed
-
- Whiteneck GG. Aging with spinal cord injury. New York: Demos Medical Publishing; 1993.
LinkOut - more resources
Full Text Sources
Other Literature Sources
