

Semaglutide, reduction in glycated haemoglobin and the risk of diabetic retinopathy
- PMID: 29178519
- PMCID: PMC5888154
- DOI: 10.1111/dom.13172
Semaglutide, reduction in glycated haemoglobin and the risk of diabetic retinopathy
Abstract
Aims: To evaluate diabetic retinopathy (DR) data from across the SUSTAIN clinical trial programme.
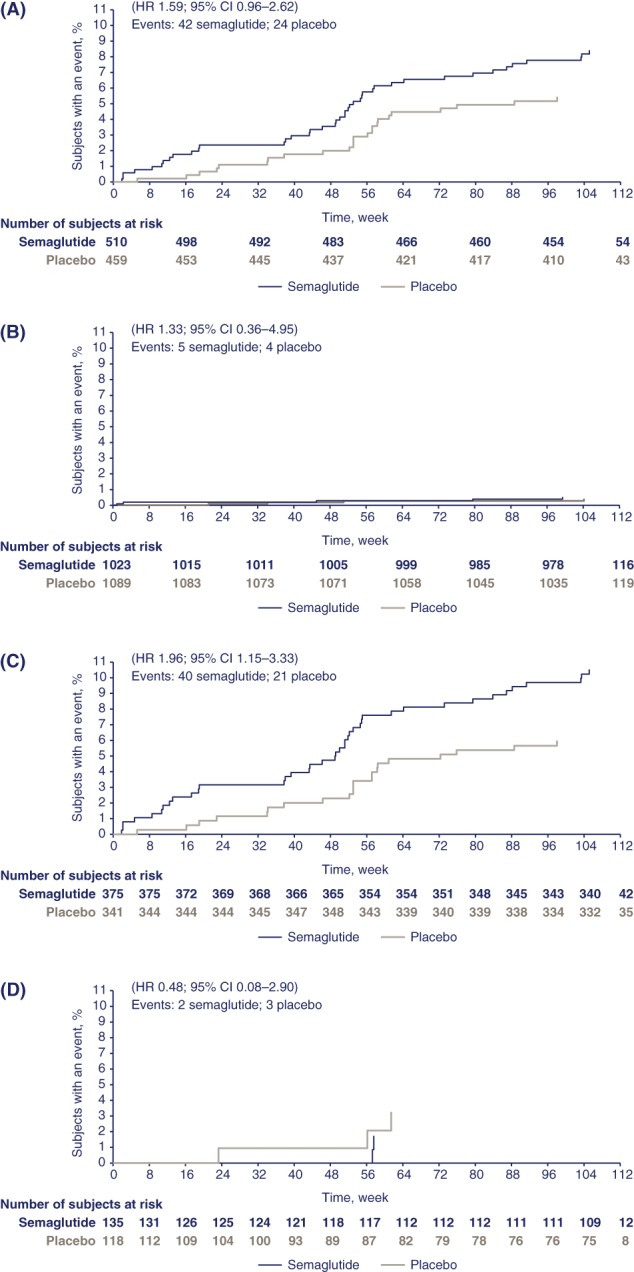
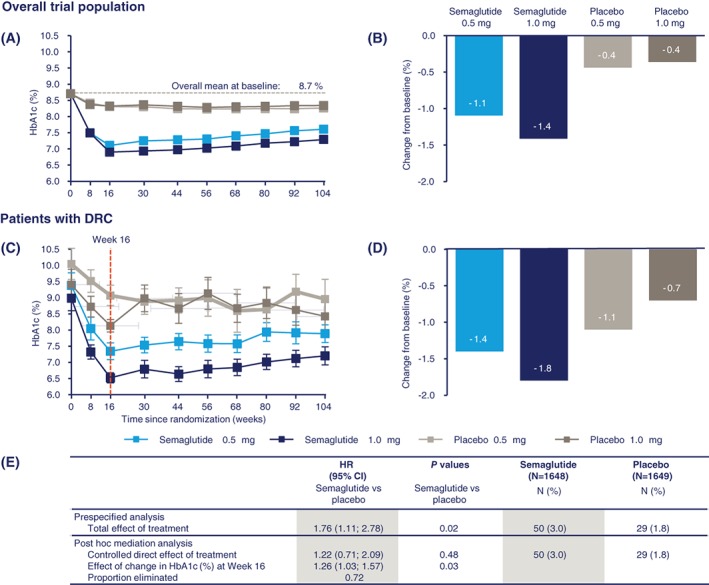
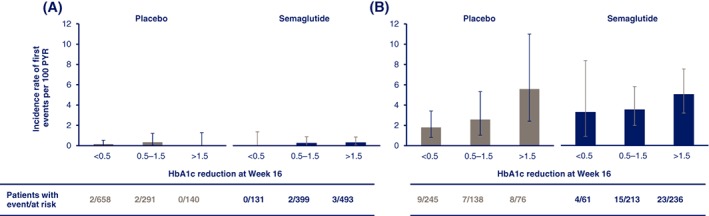
Materials and methods: The SUSTAIN clinical trial programme evaluated the efficacy and safety of semaglutide, a glucagon-like peptide-1 analogue, for the treatment of type 2 diabetes (T2D). In SUSTAIN 6, a 2-year, pre-approval cardiovascular outcomes trial, semaglutide was associated with a significant increase in the risk of DR complications (DRC) vs placebo. DR data from across the SUSTAIN trials were evaluated, and post hoc analyses of the SUSTAIN 6 data were conducted. These included subgroup analyses to identify at-risk patients and a mediation analysis with initial change in glycated haemoglobin (HbA1c; percentage-points at week 16) as a covariate, to examine the role of the magnitude of reduction in HbA1c as an intermediate factor affecting risk of DRC.
Results: There was no imbalance in DR adverse events across the SUSTAIN 1 to 5 and Japanese trials. The majority of the effect with semaglutide vs placebo in SUSTAIN 6 may be attributed to the magnitude and rapidity of HbA1c reduction during the first 16 weeks of treatment in patients who had pre-existing DR and poor glycaemic control at baseline, and who were treated with insulin.
Conclusions: Early worsening of DR is a known phenomenon associated with the rapidity and magnitude of improvement in glycaemic control with insulin; the DRC findings in SUSTAIN 6 are consistent with this. Guidance regarding the early worsening of DR is recommended with insulin. Similar recommendations may be appropriate for semaglutide.
Keywords: GLP-1 analogue; antidiabetic drug; diabetic retinopathy.
© 2017 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
T.V. declares personal fees from Amgen, Boehringer Ingelheim, Eli Lilly, AstraZeneca, Merck Sharp & Dohme, Sanofi, Novo Nordisk and Bristol‐Myers Squibb, and grants (to her institution) from Eli Lilly and Novo Nordisk. S.B. has received grants (to his institution) and personal fees from Novo Nordisk, Eli Lilly, Boehringer Ingelheim, Sanofi, Merck Sharp & Dohme, Janssen and Cellnovo. L.A.L. has received grants (to his institution) and personal fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Novo Nordisk and Sanofi, personal fees from Servier and grants (to his institution) from GlaxoSmithKline. I.L. has received grants (to her institution) and/or other fees from Novartis, GI dynamics, Pfizer, Merck and Novo Nordisk; personal fees from AstraZeneca, Sanofi and Lilly, and non‐financial (editorial) support from AstraZeneca, Sanofi, Lilly, Novo Nordisk and Boehringer Ingelheim. D.M. has received grants (to his institution) from Novo Nordisk and Takeda and reports support from Janssen, Servier and Novartis; R.S. reports grants (to his institution) and personal fees from Novo Nordisk and OM Pharma, personal fees from Bayer, and non‐financial support from Sanofi. I.C. and N.W. are full‐time employees of Novo Nordisk. M.L. reports personal fees from Novo Nordisk.
Figures
References
-
- Sorli C, Harashima SI, Tsoukas GM, et al. Efficacy and safety of once‐weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double‐blind, randomised, placebo‐controlled, parallel‐group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol. 2017;5(4):251‐260. - PubMed
-
- Ahren B, Masmiquel L, Kumar H, et al. Efficacy and safety of once‐weekly semaglutide versus once‐daily sitagliptin as an add‐on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56‐week, double‐blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017;5(5):341‐354. - PubMed
-
- Ahmann A, Capehorn M, Charpentier G, et al. Efficacy and safety of once‐weekly semaglutide vs. exenatide ER in subjects with type 2 diabetes (SUSTAIN 3). American Diabetes Association, 76th Annual Scientific Sessions; June 10‐14, 2016: New Orleans, LA.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
