

3D whole-heart phase sensitive inversion recovery CMR for simultaneous black-blood late gadolinium enhancement and bright-blood coronary CMR angiography
- PMID: 29178893
- PMCID: PMC5702978
- DOI: 10.1186/s12968-017-0405-z
3D whole-heart phase sensitive inversion recovery CMR for simultaneous black-blood late gadolinium enhancement and bright-blood coronary CMR angiography
Abstract
Background: Phase sensitive inversion recovery (PSIR) applied to late gadolinium enhancement (LGE) imaging is widely used in clinical practice. However, conventional 2D PSIR LGE sequences provide sub-optimal contrast between scar tissue and blood pool, rendering the detection of subendocardial infarcts and scar segmentation challenging. Furthermore, the acquisition of a low flip angle reference image doubles the acquisition time without providing any additional diagnostic information. The purpose of this study was to develop and test a novel 3D whole-heart PSIR-like framework, named BOOST, enabling simultaneous black-blood LGE assessment and bright-blood visualization of cardiac anatomy.
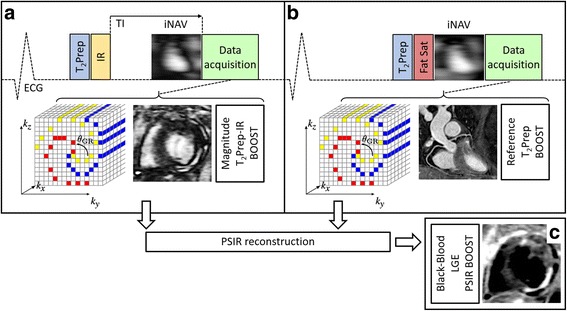
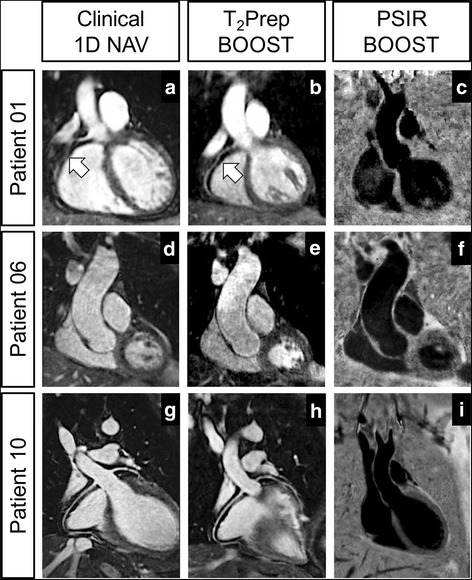
Methods: The proposed approach alternates the acquisition of a 3D volume preceded by a T2-prepared Inversion Recovery (T2Prep-IR) module (magnitude image) with the acquisition of a T2-prepared 3D volume (reference image). The two volumes (T2Prep-IR BOOST and bright-blood T2Prep BOOST) are combined in a PSIR-like reconstruction to obtain a complementary 3D black-blood volume for LGE assessment (PSIR BOOST). The black-blood PSIR BOOST and the bright-blood T2Prep BOOST datasets were compared to conventional clinical sequences for scar detection and coronary CMR angiography (CMRA) in 18 patients with a spectrum of cardiovascular disease (CVD).
Results: Datasets from 12 patients were quantitatively analysed. The black-blood PSIR BOOST dataset provided statistically improved contrast to noise ratio (CNR) between blood and scar when compared to a clinical 2D PSIR sequence (15.8 ± 3.3 and 4.1 ± 5.6, respectively). Overall agreement in LGE depiction was found between 3D black-blood PSIR BOOST and clinical 2D PSIR acquisitions, with 11/12 PSIR BOOST datasets considered diagnostic. The bright-blood T2Prep BOOST dataset provided high quality depiction of the proximal coronary segments, with improvement of visual score when compared to a clinical CMRA sequence. Acquisition time of BOOST (~10 min), providing information on both LGE uptake and heart anatomy, was comparable to that of a clinical single CMRA sequence.
Conclusions: The feasibility of BOOST for simultaneous black-blood LGE assessment and bright-blood coronary angiography was successfully tested in patients with cardiovascular disease. The framework enables free-breathing multi-contrast whole-heart acquisitions with 100% scan efficiency and predictable scan time. Complementary information on 3D LGE and heart anatomy are obtained reducing examination time.
Keywords: Black-blood; Bright-blood; Coronary MR angiography; Late gadolinium enhancement (LGE); Whole-heart.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the National Research Ethics Service and written informed consent was obtained for all the subjects. Anonymized data were analyzed at the School of Biomedical Engineering and Imaging Sciences (King’s College London) at the St. Thomas’ Hospital.
Consent for publication
All the subjects provided written informed consent for the publication of accompanying images in this manuscript. The consent forms are held in the patients’ clinical notes and are available to the Editor-in-Chief upon request.
Competing interests
R.N. is employed by Siemens Healthcare Limited. All the other Authors declare that they do not have competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures





References
-
- Abdel-Aty H, Boye P, Zagrosek A, Wassmuth R, Kumar A, Messroghli D, Bock P, Dietz R, Friedrich MG, Schulz-Menger J. Diagnostic performance of cardiovascular magnetic resonance in patients with suspected acute myocarditis: comparison of different approaches. J Am Coll Cardiol. 2005;45:1815–1822. doi: 10.1016/j.jacc.2004.11.069. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
