

High-volume hemofiltration in adult burn patients with septic shock and acute kidney injury: a multicenter randomized controlled trial
- PMID: 29178943
- PMCID: PMC5702112
- DOI: 10.1186/s13054-017-1878-8
High-volume hemofiltration in adult burn patients with septic shock and acute kidney injury: a multicenter randomized controlled trial
Abstract
Background: Sepsis and septic shock occur commonly in severe burns. Acute kidney injury (AKI) is also common and often results as a consequence of sepsis. Mortality is unacceptably high in burn patients who develop AKI requiring renal replacement therapy and is presumed to be even higher when combined with septic shock. We hypothesized that high-volume hemofiltration (HVHF) as a blood purification technique would be beneficial in this population.
Methods: We conducted a multicenter, prospective, randomized, controlled clinical trial to evaluate the impact of HVHF on the hemodynamic profile of burn patients with septic shock and AKI involving seven burn centers in the United States. Subjects randomized to the HVHF were prescribed a dose of 70 ml/kg/hour for 48 hours while control subjects were managed in standard fashion in accordance with local practices.
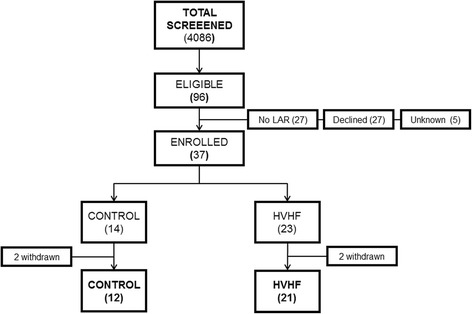
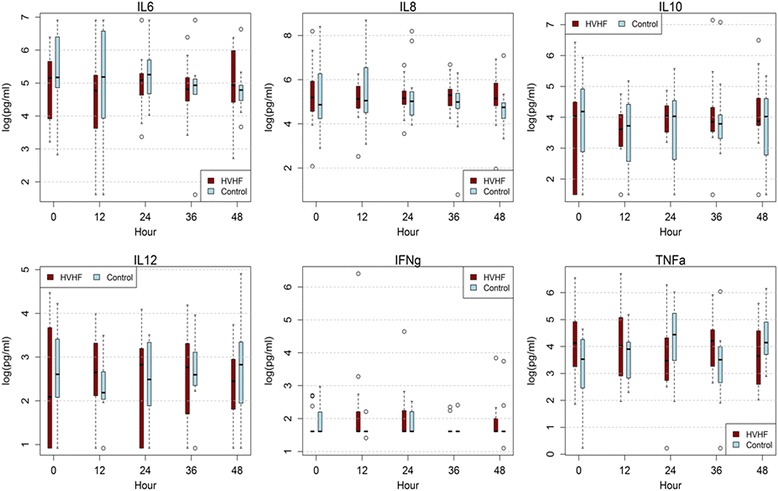
Results: During a 4-year period, a total of nine subjects were enrolled for the intervention during the ramp-in phase and 28 subjects were randomized, 14 each into the control and HVHF arms respectively. The study was terminated due to slow enrollment. Ramp-in subjects were included along with those randomized in the final analysis. Our primary endpoint, the vasopressor dependency index, decreased significantly at 48 hours compared to baseline in the HVHF group (p = 0.007) while it remained no different in the control arm. At 14 days, the multiple organ dysfunction syndrome score decreased significantly in the HVHF group when compared to the day of treatment initiation (p = 0.02). No changes in inflammatory markers were detected during the 48-hour intervention period. No significant difference in survival was detected. No differences in adverse events were noted between the groups.
Conclusions: HVHF was effective in reversing shock and improving organ function in burn patients with septic shock and AKI, and appears safe. Whether reversal of shock in these patients can improve survival is yet to be determined.
Trial registration: Clinicaltrials.gov NCT01213914 . Registered 30 September 2010.
Keywords: Acute kidney injury; Burns; High-volume hemofiltration; Multicenter; Randomized controlled trial; Septic shock.
Conflict of interest statement
Authors’ information
Not applicable.
Ethic
The study was approved in a multilevel institutional review process. The core protocol was initially reviewed by the United States Army Medical Research and Materiel Command (USAMRMC) Institutional Review Board (IRB) and reviewed again for final approval by the Army Human Research Protection Office (AHRPO). The core protocol was then submitted to each participating site’s local IRB with site-specific addendums and approved again by AHRPO. All amendments to the core protocol required multilevel review with final approval by the AHRPO. A list of IRBs for each specific site is listed in Additional file 1. Informed consent was obtained from all participating subjects through their surrogates.
Consent for publication
All authors gave final approval of the final manuscript to be published.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
