

Traditional Chinese medicine Danggui Buxue Tang inhibits colorectal cancer growth through induction of autophagic cell death
- PMID: 29179457
- PMCID: PMC5687627
- DOI: 10.18632/oncotarget.19902
Traditional Chinese medicine Danggui Buxue Tang inhibits colorectal cancer growth through induction of autophagic cell death
Abstract
Purpose: The induction of autophagic cell death is an important process in the development of anticancer therapeutics. We aimed to evaluate the activity of the ancient Chinese decoction Danggui Buxue Tang (DBT) against colorectal cancer (CRC) and the associated autophagy-related mechanism.
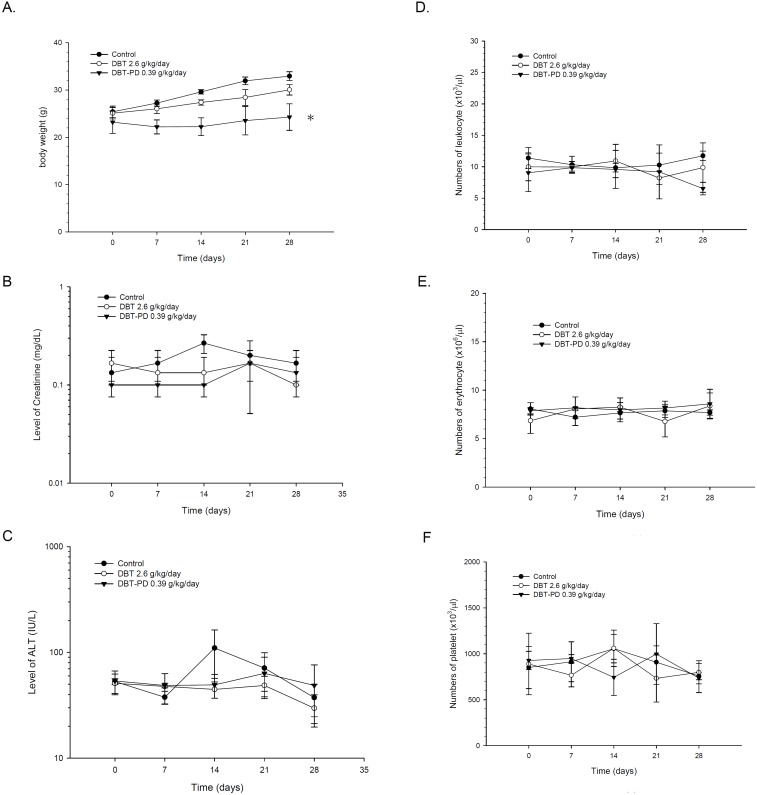
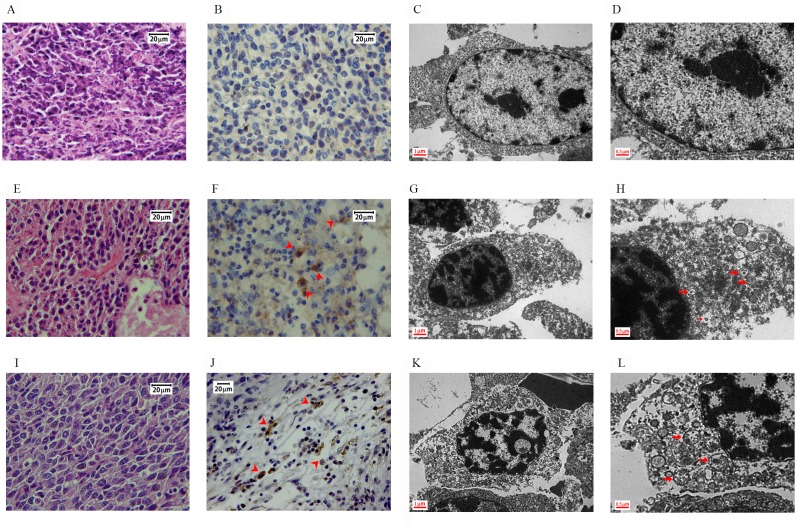
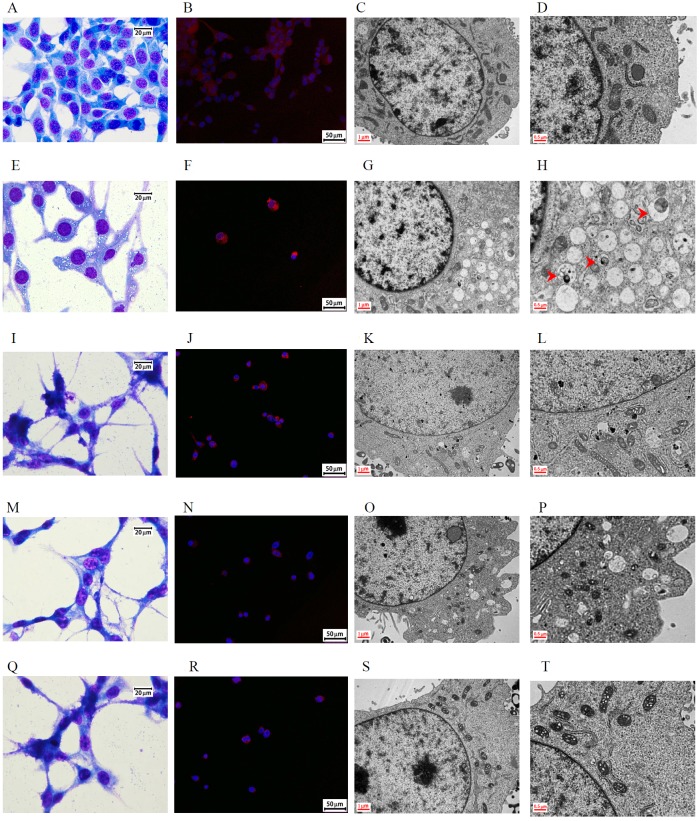
Materials and methods: CT26 CRC cells were implanted into syngeneic BALB/c mice for the tumor growth assay. DBT extracts and DBT-PD (polysaccharide-depleted) fractions were orally administered. The toxicity profiles of the extracts were analyzed using measurements of body weight, hemogram, and biochemical parameters. The morphology of tissue sections was observed using light and transmission electron microscopy. Western blotting and small interference RNA assays were used to determine the mechanism.
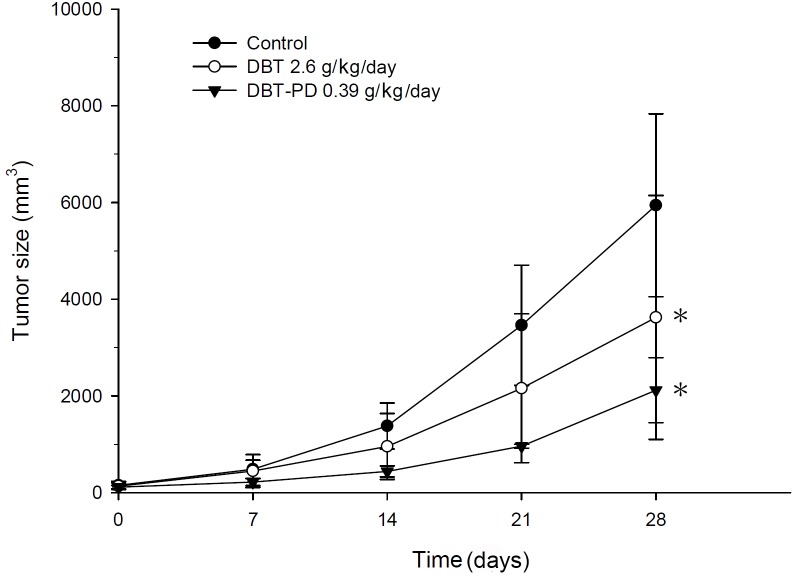
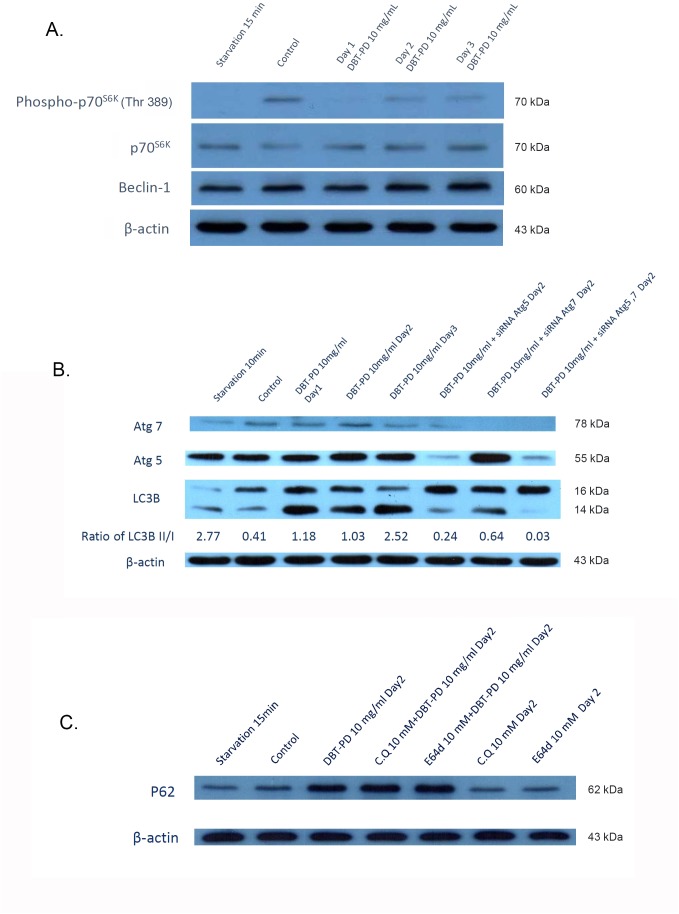
Results: DBT-PD and DBT, which contained an equal amount of DBT-PD, inhibited CT26 syngeneic tumor growth. In the tumor specimen, the expression of microtubule-associated proteins 1A/1B light chain 3B (LC3B) was upregulated by DBT-PD and DBT. The development of autophagosomes was observed via transmission electron microscopy in tumors treated with DBT-PD and DBT. In vitro experiments for mechanism clarification demonstrated that DBT-PD could induce autophagic death in CT26 cells accompanied by LC3B lipidation, downregulation of phospho-p70s6k, and upregulation of Atg7. RNA interference of Atg7, but not Atg5, partially reversed the effect of DBT-PD on LC3B lipidation and expression of phospho-p70s6k and Atg7. The changes in ultrastructural morphology and LC3B expression induced by DBT-PD were also partially blocked by the knockdown of Atg7 mRNA.
Conclusion: DBT induced autophagic death of colorectal cancer cells through the upregulation of Atg7 and modulation of the mTOR/p70s6k signaling pathway.
Keywords: Danggui Buxue Tang; autophagy; colorectal cancer; mammalian target of rapamycin (mTOR); traditional Chinese medicine.
Conflict of interest statement
CONFLICTS OF INTEREST The authors declare no conflicts of interest.
Figures
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Eddy DM. Screening for colorectal cancer. Ann Intern Med. 1990;113:373–384. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Center MM, Jemal A, Smith RA, Ward E. Worldwide variations in colorectal cancer. CA Cancer J Clin. 2009;59:366–378. - PubMed
-
- O'Connell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst. 2004;96:1420–1425. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
