

Gastrointestinal tuberculosis following renal transplantation accompanied with septic shock and acute respiratory distress syndrome: a survival case presentation
- PMID: 29179699
- PMCID: PMC5704353
- DOI: 10.1186/s12876-017-0695-5
Gastrointestinal tuberculosis following renal transplantation accompanied with septic shock and acute respiratory distress syndrome: a survival case presentation
Abstract
Background: Post-transplant tuberculosis (PTTB) is a serious opportunistic infection in renal graft recipients with a 30-70 fold higher incidence compared to the general population. PTTB occurs most frequently within the first years after transplantation, manifesting as pulmonary or disseminated TB. Gastrointestinal TB (GITB) is a rare and potentially lethal manifestation of PTTB and may show delayed onset in renal transplant recipients due to the use of lower doses of immunosuppressants. Further, non-specificity of symptoms and the common occurrence of GI disorders in transplant recipients may delay diagnosis of GITB.
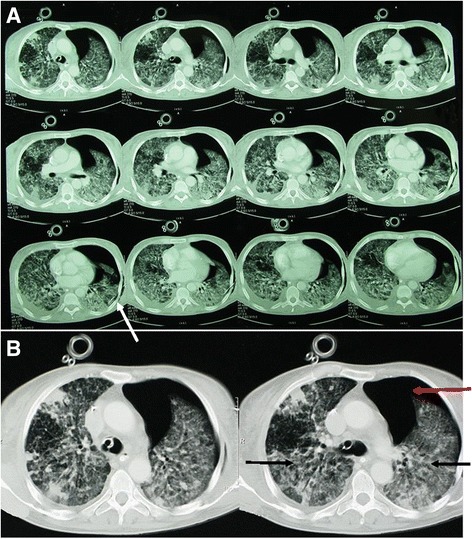
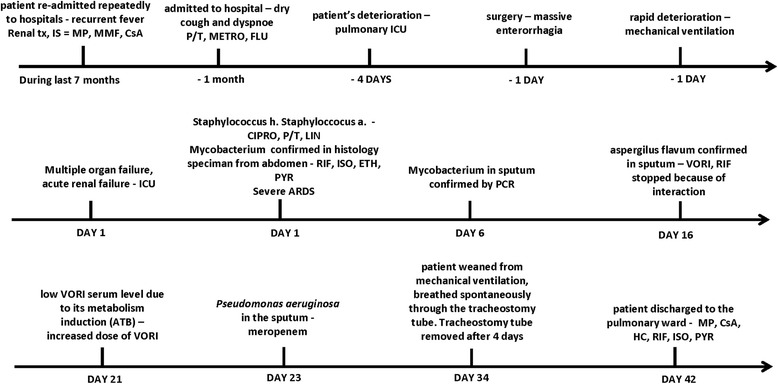
Case presentation: Here we report a rare survival case of isolated GITB in a renal transplant recipient, occurring seven years after transplantation. The patient's condition was complicated by severe sepsis with positive blood culture Staphylococcus haemolyticus, septic shock, multiple organ failure including acute respiratory distress syndrome (ARDS) and acute renal failure, requiring mechanical ventilation, vasopressor circulatory support and intermittent hemodialysis. Furthermore, nosocomial infections such as invasive aspergillosis and Pseudomonas aeruginosa occurred during hospitalization. Antituberculosis therapy (rifampicin, isoniazid, ethambutol and pyrazinamide) was initiated upon Mycobacterium confirmation. Moreover, treatment with voriconazole due to the Aspergillus flavus and meropenem due to the Pseudomonas aeruginosa was initiated, the former necessitating discontinuation of rifampicin. After 34 days, the patient was weaned from mechanical ventilation and was discharged to the pulmonary ward, followed by complete recovery.
Conclusion: This case offers a guideline for the clinical management towards survival of GITB in transplant patients, complicated by septic shock and multiple organ failure, including acute renal injury and ARDS.
Keywords: Acute respiratory distress syndrome; Gastrointestinal tuberculosis; Multiple organ failure; Renal transplantation; Septic shock.
Conflict of interest statement
Ethics approval and consent to participate
The methods were carried out in accordance with the principles stated in the Declaration of Helsinki. As a case presentation, this study does not need ethical approval (Not applicable).
Written informed consent was obtained from patient who participated in the study. The consent form is held by the authors and is available for review by the Editor-in-Chief. No organs/tissues were obtained from prisoners and organs were obtained via Department of Urology with Kidney Transplant Center, University Hospital Bratislava, Bratislava, Slovak Republic.
Consent for publication
Written informed consent was obtained from the patient for publication of their individual details and accompanying images in this manuscript. The consent form is held by the authors and is available for review by the Editor-in-Chief.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
