

Segmental Sclerosis and Extracapillary Hypercellularity Predict Diabetic ESRD
- PMID: 29180393
- PMCID: PMC5791055
- DOI: 10.1681/ASN.2017020192
Segmental Sclerosis and Extracapillary Hypercellularity Predict Diabetic ESRD
Abstract
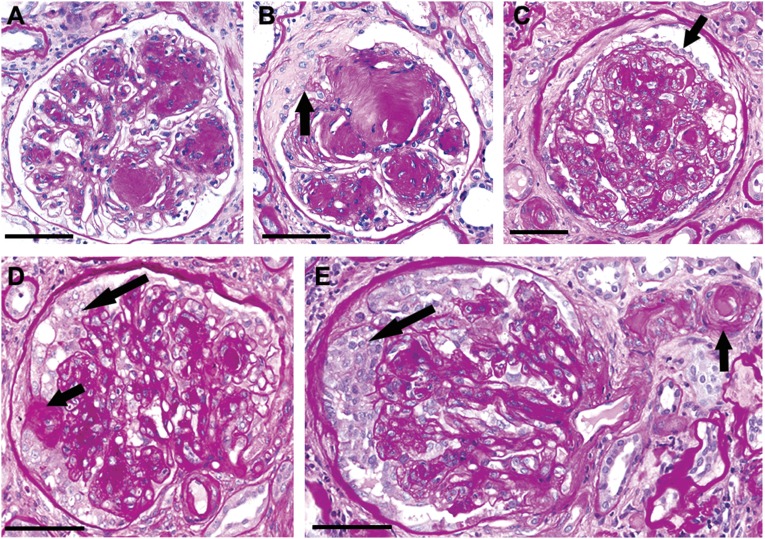
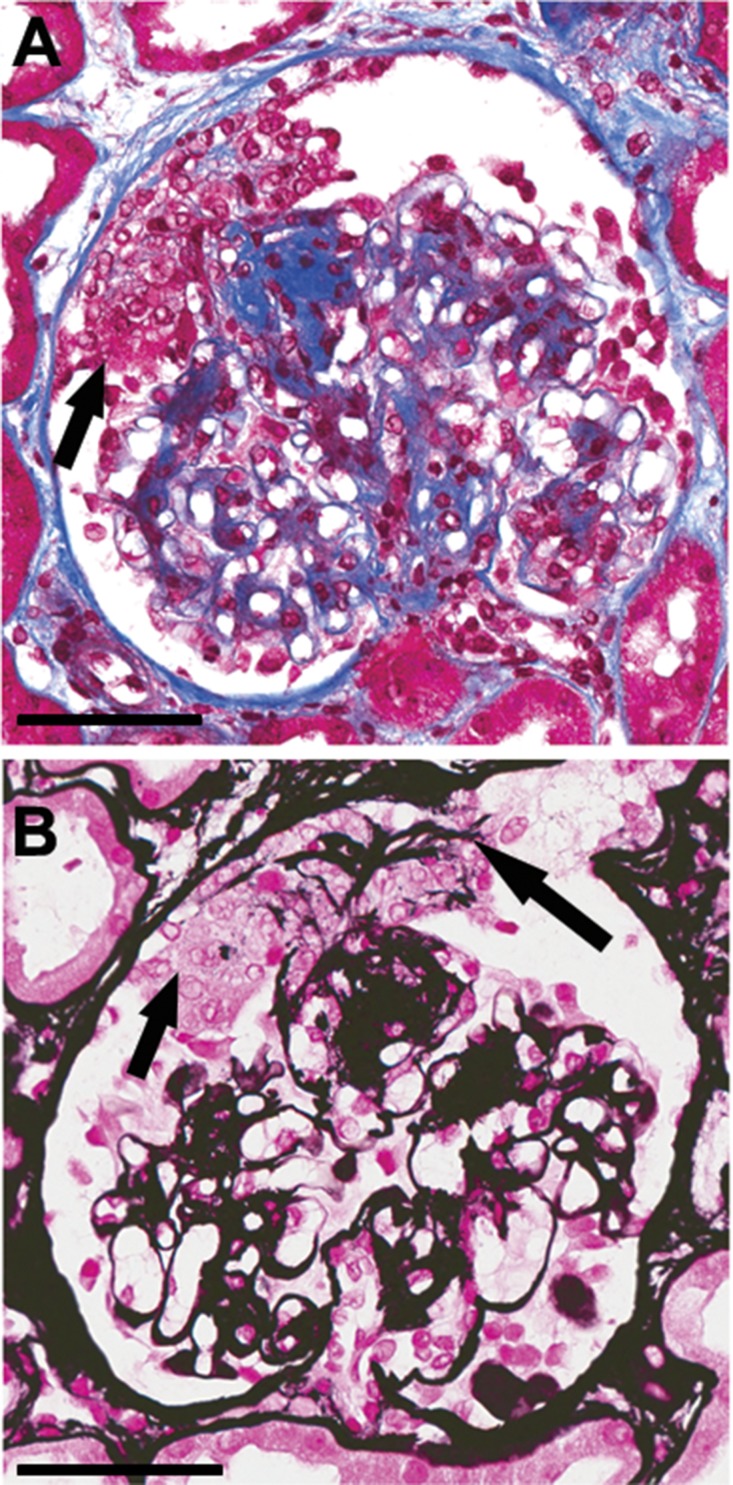
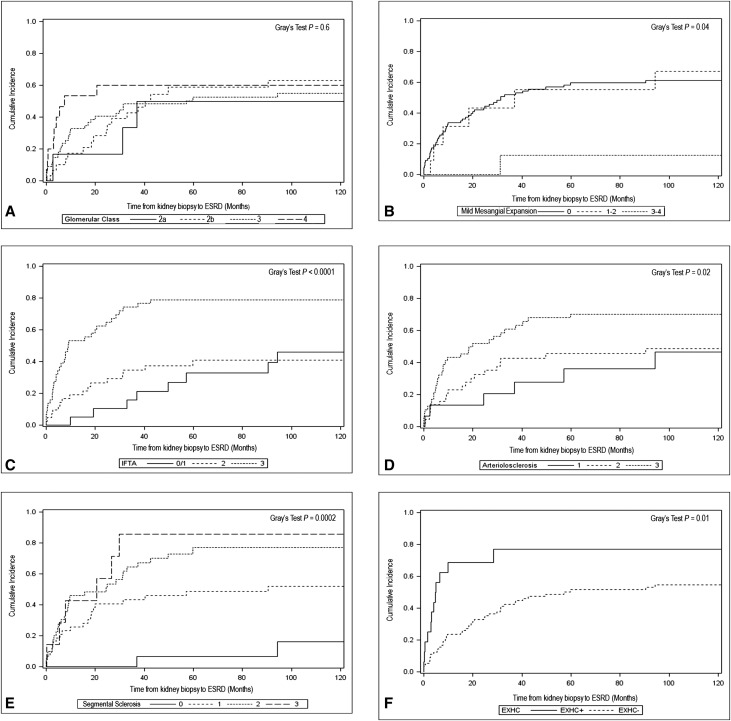
Pathogenetic markers of diabetic kidney disease (DKD) progression to ESRD are lacking. We characterized the prognostic value of histologic findings in DKD for time to ESRD in native kidney specimens from biopsies performed from 1995 to 2011 with diabetic glomerulosclerosis as the only glomerular disease diagnosis (n=109). Biopsy specimens were analyzed according to standard methods, including determination of diabetic nephropathy class, as defined by the Renal Pathology Society. Clinical data were extracted from electronic medical records. We used competing risk models, with death as the competing risk, to estimate subdistribution hazard ratios (HRs) for ESRD. All multivariable models included age, sex, black race, baseline eGFR, and baseline proteinuria. Pathologic characteristics achieving P<0.1 were added into successively complex models. ESRD occurred in 56% of patients, and 26% of patients died before reaching ESRD. In univariate analyses, diabetic nephropathy class was not statistically significant in predicting time to ESRD. The final multivariable model (n=106) showed a borderline association between mild mesangial expansion and decreased risk for ESRD (subdistribution HR, 0.64; 95% confidence interval, 0.40 to 1.00). Poor prognostic factors in the final model included segmental sclerosis and extracapillary hypercellularity (subdistribution HR, 2.04; 95% confidence interval, 1.36 to 3.05; and subdistribution HR, 2.21; 95% confidence interval, 1.19 to 4.11, respectively). In conclusion, we identified segmental sclerosis and extracapillary hypercellularity as novel, poor prognostic indicators of time from DKD to ESRD. Whether these indicators represent a distinct pathogenetic phenotype of DKD will require a large study with a broad spectrum of disease severity.
Keywords: diabetic glomerulosclerosis; end stage; extracapillary hypercellularity; pathology; renal disease; segmental sclerosis.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- United States Renal Data System : USRDS 2016 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institute of Diabetes and Digestive and Kidney Diseases, 2016
-
- Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR; UKPDS Study Group : Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes study 74. Diabetes 55: 1832–1839, 2006 - PubMed
-
- Packham DK, Alves TP, Dwyer JP, Atkins R, de Zeeuw D, Cooper M, Shahinfar S, Lewis JB, Lambers Heerspink HJ: Relative incidence of ESRD versus cardiovascular mortality in proteinuric type 2 diabetes and nephropathy: Results from the DIAMETRIC (Diabetes Mellitus Treatment for Renal Insufficiency Consortium) database. Am J Kidney Dis 59: 75–83, 2012 - PubMed
-
- Ivory SE, Packham DK, Reutens AT, Wolfe R, Rohde RD, Lewis J, Atkins RC; Collaborative Study Group : Residual proteinuria and eGFR predict progression of renal impairment within 2 years in type 2 diabetic patients with nephropathy who are receiving optimal treatment with angiotensin receptor blockers. Nephrology (Carlton) 18: 516–524, 2013 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
