

Clinical Outcomes After Ablation of the AV Junction in Patients With Atrial Fibrillation: Impact of Cardiac Resynchronization Therapy
- PMID: 29180458
- PMCID: PMC5779040
- DOI: 10.1161/JAHA.117.007270
Clinical Outcomes After Ablation of the AV Junction in Patients With Atrial Fibrillation: Impact of Cardiac Resynchronization Therapy
Abstract
Background: Patients with atrial fibrillation (AF) often undergo AV junction ablation (AVJA) and pacemaker implantation. Right ventricular (RV) pacing contributes to increased risk of heart failure (HF), which may be mitigated by biventricular pacing. We sought to determine the impact of AVJA concurrent with RV versus biventricular pacemaker implantation on AF and HF hospitalizations.
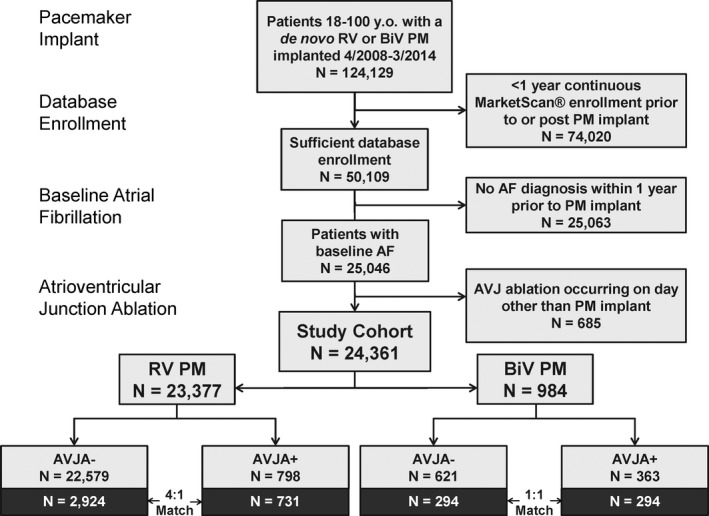
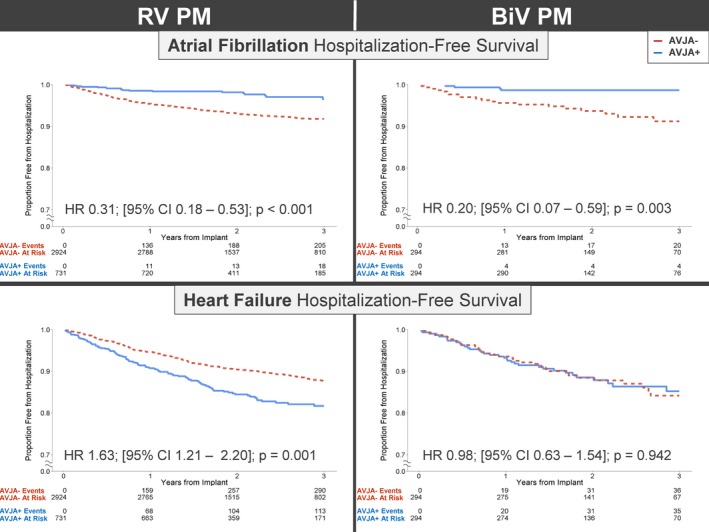
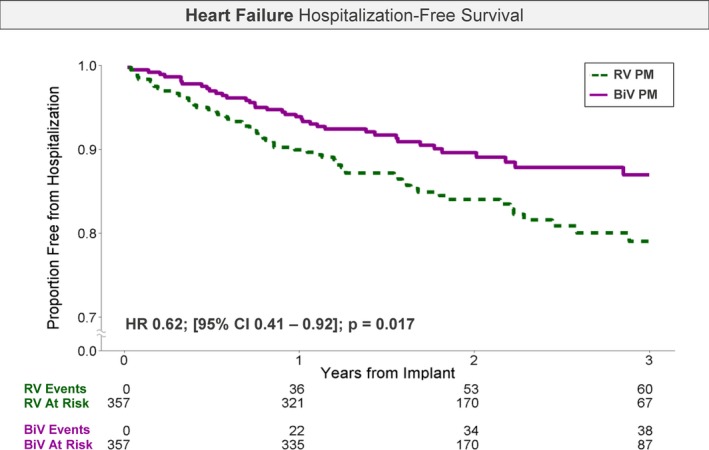
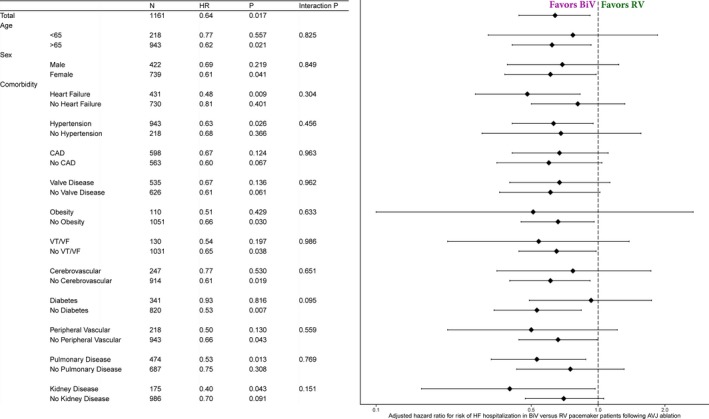
Methods and results: The MarketScan Commercial and Medicare Supplemental claims database was used to select 18- to 100-year-old patients with AF with pacemaker implantation. Patients were divided into those with an RV and a biventricular pacemaker and further into those who did (AVJA+) or did not undergo concurrent ablation. Separately, the AVJA+ group was divided into those receiving RV versus biventricular pacemakers. AF and HF hospitalization rates were compared between groups after matching on demographics, comorbidities, and baseline hospitalization rates. The study included 24 361 patients, with RV (n=23 377) or biventricular (n=984) pacemakers; 1611 patients underwent AVJA. AVJA+ was associated with reduced AF hospitalization risk (RV hazard ratio [HR], 0.31; P<0.001; biventricular HR, 0.20; P=0.003) compared with no AVJA. However, HF hospitalization risk was increased for RV (HR, 1.63; P=0.001), but not biventricular (HR, 0.98; P=0.942), pacemakers. In AVJA+ patients, biventricular pacing was associated with reduced risk of HF hospitalization versus RV pacing (HR, 0.62; P=0.017).
Conclusions: In a large cohort of patients with AF, AVJA+ significantly reduced AF hospitalizations, irrespective of whether an RV or a biventricular pacemaker was implanted. However, AVJA was associated with a marked HF hospitalization increase in patients with an RV pacemaker, which was ameliorated with biventricular pacing.
Keywords: ablation; atrial fibrillation; biventricular pacing; heart failure; pacemaker.
© 2017 The Authors and Abbott. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

References
-
- Wood MA, Brown‐Mahoney C, Kay GN, Ellenbogen KA. Clinical outcomes after ablation and pacing therapy for atrial fibrillation: a meta‐analysis. Circulation. 2000;101:1138–1144. - PubMed
-
- Merchant FM, Hoskins MH, Musat DL, Prillinger JB, Roberts GJ, Nabutovsky Y, Mittal S. Incidence and time course for developing heart failure with high‐burden right ventricular pacing. Circ Cardiovasc Qual Outcomes. 2017;10:e003564. - PubMed
-
- Doshi RN, Daoud EG, Fellows C, Turk K, Duran A, Hamdan MH, Pires LA; for the PAVE Study Group. Left ventricular‐based cardiac stimulation Post AV Nodal Ablation Evaluation (The PAVE Study). J Cardiovasc Electrophysiol. 2005;16:1160–1165. - PubMed
-
- Brignole M, Botto G, Mont L, Iacopino S, De Marchi G, Oddone D, Luzi M, Tolosana JM, Navazio A, Menozzi C. Cardiac resynchronization therapy in patients undergoing atrioventricular junction ablation for permanent atrial fibrillation: a randomized trial. Eur Heart J. 2011;32:2420–2429. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
