

Integrated Resistance Analysis of CERTAIN-1 and CERTAIN-2 Studies in Hepatitis C Virus-Infected Patients Receiving Glecaprevir and Pibrentasvir in Japan
- PMID: 29180522
- PMCID: PMC5786793
- DOI: 10.1128/AAC.02217-17
Integrated Resistance Analysis of CERTAIN-1 and CERTAIN-2 Studies in Hepatitis C Virus-Infected Patients Receiving Glecaprevir and Pibrentasvir in Japan
Abstract
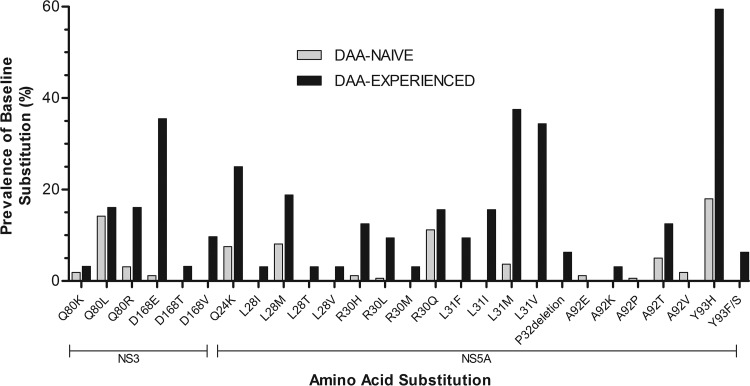
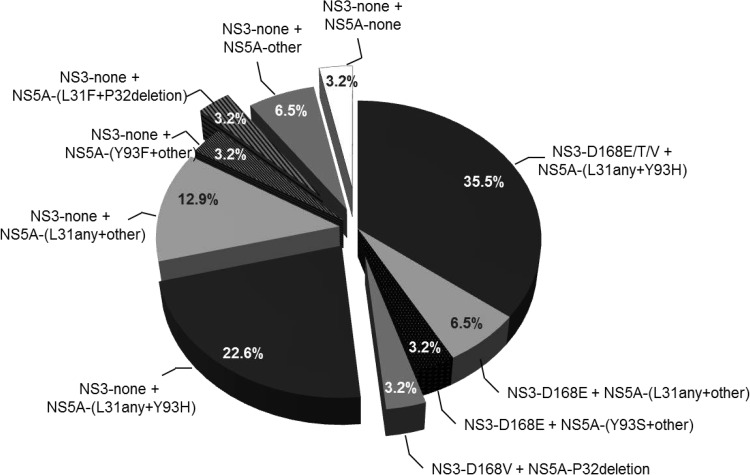
Glecaprevir and pibrentasvir are hepatitis C virus (HCV) pangenotypic inhibitors targeting NS3/4A protease and NS5A, respectively. This once-daily, fixed-dose combination regimen demonstrated high sustained virologic response 12 weeks postdosing (SVR12) rates in CERTAIN-1 and CERTAIN-2 studies in Japanese HCV-infected patients, with a low virologic failure rate (1.2%). There were no virologic failures among direct-acting antiviral (DAA)-treatment-naive genotype 1a (GT1a) (n = 4)-, GT1b (n = 128)-, and GT2 (n = 97)-infected noncirrhotic patients treated for 8 weeks or among GT1b (n = 38)- or GT2 (n = 20)-infected patients with compensated cirrhosis treated for 12 weeks. Two of 33 DAA-experienced and 2 of 12 GT3-infected patients treated for 12 weeks experienced virologic failure. Pooled resistance analysis, grouped by HCV subtype, treatment duration, prior treatment experience, and cirrhosis status, was conducted. Among DAA-naive GT1b-infected patients, the baseline prevalence of NS3-D168E was 1.2%, that of NS5A-L31M was 3.6%, and that of NS5A-Y93H was 17.6%. Baseline polymorphisms in NS3 or NS5A were less prevalent in GT2, with the exception of the common L/M31 polymorphism in NS5A. Among DAA-experienced GT1b-infected patients (30/32 daclatasvir plus asunaprevir-experienced patients), the baseline prevalence of NS3-D168E/T/V was 48.4%, that of NS5A-L31F/I/M/V was 81.3%, that of the NS5A P32deletion was 6.3%, and that of NS5A-Y93H was 59.4%. Common baseline polymorphisms in NS3 and/or NS5A had no impact on treatment outcomes in GT1- and GT2-infected patients; the impact on GT3-infected patients could not be assessed due to the enrollment of patients infected with diverse subtypes and the limited number of patients. The glecaprevir-pibrentasvir combination regimen allows a simplified treatment option without the need for HCV subtyping or baseline resistance testing for DAA-naive GT1- or GT2-infected patients. (The CERTAIN-1 and CERTAIN-2 studies have been registered at ClinicalTrials.gov under identifiers NCT02707952 and NCT02723084, respectively.).
Keywords: HCV; NS5A inhibitor; glecaprevir; pibrentasvir; protease inhibitors.
Copyright © 2018 Krishnan et al.
Figures
References
-
- World Health Organization. 2017. Global hepatitis report 2017. World Health Organization, Geneva, Switzerland.
-
- Hayashi K, Fukuda Y, Nakano I, Katano Y, Toyoda H, Yokozaki S, Hayakawa T, Morita K, Nishimura D, Kato K, Urano F, Takamatsu J. 2003. Prevalence and characterization of hepatitis C virus genotype 4 in Japanese hepatitis C carriers. Hepatol Res 25:409–414. doi:10.1016/S1386-6346(03)00016-0. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
