

Classifying Colorectal Cancer by Tumor Location Rather than Sidedness Highlights a Continuum in Mutation Profiles and Consensus Molecular Subtypes
- PMID: 29180604
- PMCID: PMC5844818
- DOI: 10.1158/1078-0432.CCR-17-2484
Classifying Colorectal Cancer by Tumor Location Rather than Sidedness Highlights a Continuum in Mutation Profiles and Consensus Molecular Subtypes
Abstract
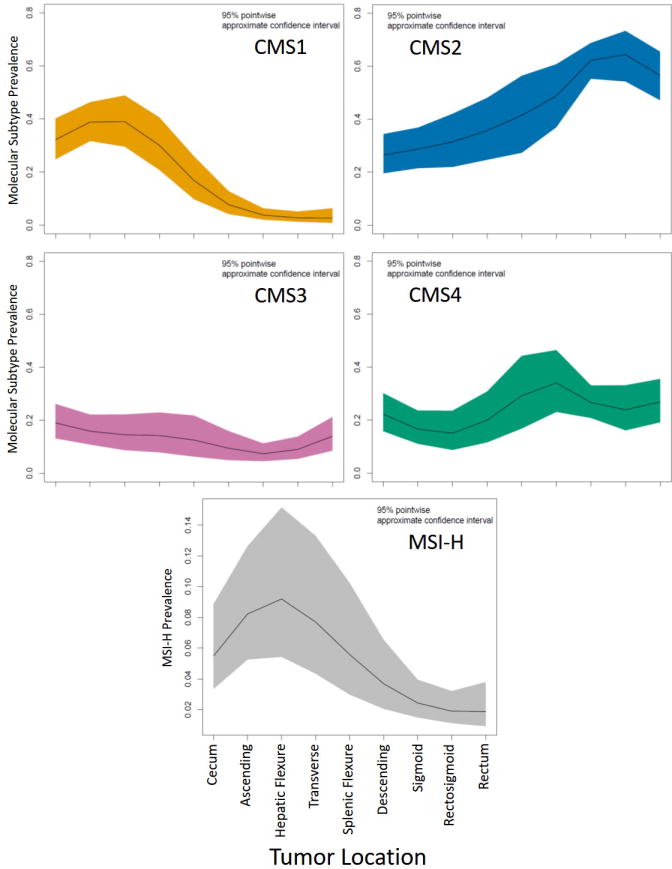
Purpose: Colorectal cancers are classified as right/left-sided based on whether they occur before/after the splenic flexure, with established differences in molecular subtypes and outcomes. However, it is unclear if this division is optimal and whether precise tumor location provides further information.Experimental Design: In 1,876 patients with colorectal cancer, we compared mutation prevalence and overall survival (OS) according to side and location. Consensus molecular subtype (CMS) was compared in a separate cohort of 608 patients.Results: Mutation prevalence differed by side and location for TP53, KRAS, BRAFV600, PIK3CA, SMAD4, CTNNB1, GNAS, and PTEN Within left- and right-sided tumors, there remained substantial variations in mutation rates. For example, within right-sided tumors, RAS mutations decreased from 70% for cecal, to 43% for hepatic flexure location (P = 0.0001), while BRAFV600 mutations increased from 10% to 22% between the same locations (P < 0.0001). Within left-sided tumors, the sigmoid and rectal region had more TP53 mutations (P = 0.027), less PIK3CA (P = 0.0009), BRAF (P = 0.0033), or CTNNB1 mutations (P < 0.0001), and less MSI (P < 0.0001) than other left-sided locations. Despite this, a left/right division preceding the transverse colon maximized prognostic differences by side and transverse colon tumors had K-modes mutation clustering that appeared more left than right sided. CMS profiles showed a decline in CMS1 and CMS3 and rise in CMS2 prevalence moving distally.Conclusions: Current right/left classifications may not fully recapitulate regional variations in tumor biology. Specifically, the sigmoid-rectal region appears unique and the transverse colon is distinct from other right-sided locations. Clin Cancer Res; 24(5); 1062-72. ©2017 AACRSee related commentary by Dienstmann, p. 989.
©2017 American Association for Cancer Research.
Conflict of interest statement
Figures



Comment in
-
Tumor Side as Model of Integrative Molecular Classification of Colorectal Cancer.Clin Cancer Res. 2018 Mar 1;24(5):989-990. doi: 10.1158/1078-0432.CCR-17-3477. Epub 2017 Dec 21. Clin Cancer Res. 2018. PMID: 29269378
References
-
- Holch JW, Ricard I, Stintzing S, Modest DP, Heinemann V. The relevance of primary tumour location in patients with metastatic colorectal cancer: A meta-analysis of first-line clinical trials. Eur J Cancer [Internet] 2017;70:87–98. Available from: http://dx.doi.org/10.1016/j.ejca.2016.10.007. - DOI - PubMed
-
- Tran B, Kopetz S, Tie J, Gibbs P, Jiang ZQ, Lieu CH, et al. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer [Internet] 2011;117:4623–32. Available from: http://doi.wiley.com/10.1002/cncr.26086. - DOI - PMC - PubMed
-
- Guinney J, Dienstmann R, Wang X, de Reyniès A, Schlicker A, Soneson C, et al. The consensus molecular subtypes of colorectal cancer. Nat Med [Internet] 2015;21:1350–6. Available from: http://www.nature.com/doifinder/10.1038/nm.3967. - DOI - PMC - PubMed
-
- Cha Y, Kim K-J, Han S-W, Rhee YY, Bae JM, Wen X, et al. Adverse prognostic impact of the CpG island methylator phenotype in metastatic colorectal cancer. Br J Cancer [Internet] 2016;115:164–71. Available from: http://dx.doi.org/10.1038/bjc.2016.176. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
