

Clinical Implication of Mycophenolic Acid Trough Concentration Monitoring in Kidney Transplant Patients on a Tacrolimus Triple Maintenance Regimen: A Single-Center Experience
- PMID: 29180612
- PMCID: PMC6248041
- DOI: 10.12659/aot.906041
Clinical Implication of Mycophenolic Acid Trough Concentration Monitoring in Kidney Transplant Patients on a Tacrolimus Triple Maintenance Regimen: A Single-Center Experience
Abstract
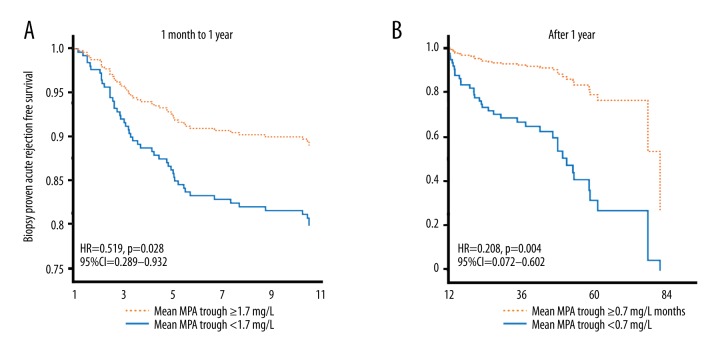
BACKGROUND This study was designed to analyze the clinical implications of mycophenolic acid trough concentration monitoring. MATERIAL AND METHODS We collected data of patients with mycophenolic acid trough concentration monitoring after their first kidney transplant between November 2006 and March 2015 who were prescribed tacrolimus, mycophenolate, and methylprednisolone. Analyses were performed on 3 periods: 1 month, 1 month to 1 year, and after 1 year post-transplantation. To analyze factors related to acute cellular rejection, logistic regression was used for 1 month, while Cox analysis was used during 1 month to 1 year and after 1 year post-transplantation. RESULTS In the 145 patients receiving mycophenolate mofetil, mean tacrolimus trough ≥7.0 ng/mL (OR=0.177, CI=0.060-0.524, p=0.002) and mean mycophenolic acid trough ≥1.7 mg/L (OR=0.190, CI=0.040-0.896, p=0.036) were protective for rejection during 1 month. Mean mycophenolic acid trough ≥1.7 mg/L (HR=0.179, CI=0.040-0.806, p=0.025) and ≥0.7 mg/L (HR=0.142, CI=0.028-0.729, p=0.019) were related to better rejection-free survival during 1 month to 1 year and after 1 year, respectively. In 399 patients receiving enteric-coated mycophenolate sodium, mean tacrolimus trough ≥7.0 ng/mL (OR=0.258, CI=0.131-0.507, p<0.001) and mean mycophenolic acid trough ≥2.1 mg/L (OR=0.507, CI=0.264-0.973, p=0.041) were protective for rejection during 1 month. Mean mycophenolic acid trough ≥1.7 mg/L (HR=0.519, CI=0.289-0.932, p=0.028) and ≥0.7 mg/L (HR=0.208, CI=0.072-0.602, p=0.004) were related to better rejection-free survival during 1 month to 1 year and after 1 year, respectively. CONCLUSIONS Mycophenolic acid trough concentration monitoring can be useful in preventing acute cellular rejection in patients receiving tacrolimus, mycophenolate, and methylprednisolone.
Conflict of interest statement
None.
Figures


References
-
- Staatz CE, Tett SE. Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin Pharmacokinet. 2007;46:13–58. - PubMed
-
- Arns W, Breuer S, Choudhury S, et al. Enteric-coated mycophenolate sodium delivers bioequivalent MPA exposure compared with mycophenolate mofetil. Clin Transplant. 2005;19:199–206. - PubMed
-
- Bullingham RE, Nicholls AJ, Kamm BR. Clinical pharmacokinetics of mycophenolate mofetil. Clin Pharmacokinet. 1998;34:429–55. - PubMed
-
- Knight SR, Morris PJ. Does the evidence support the use of mycophenolate mofetil therapeutic drug monitoring in clinical practice? A systematic review. Transplantation. 2008;85:1675–85. - PubMed
-
- Hale MD, Nicholls AJ, Bullingham RE, et al. The pharmacokinetic-pharmacodynamic relationship for mycophenolate mofetil in renal transplantation. Clin Pharmacol Ther. 1998;64:672–83. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
