

Integrating evolutionary dynamics into treatment of metastatic castrate-resistant prostate cancer
- PMID: 29180633
- PMCID: PMC5703947
- DOI: 10.1038/s41467-017-01968-5
Integrating evolutionary dynamics into treatment of metastatic castrate-resistant prostate cancer
Abstract
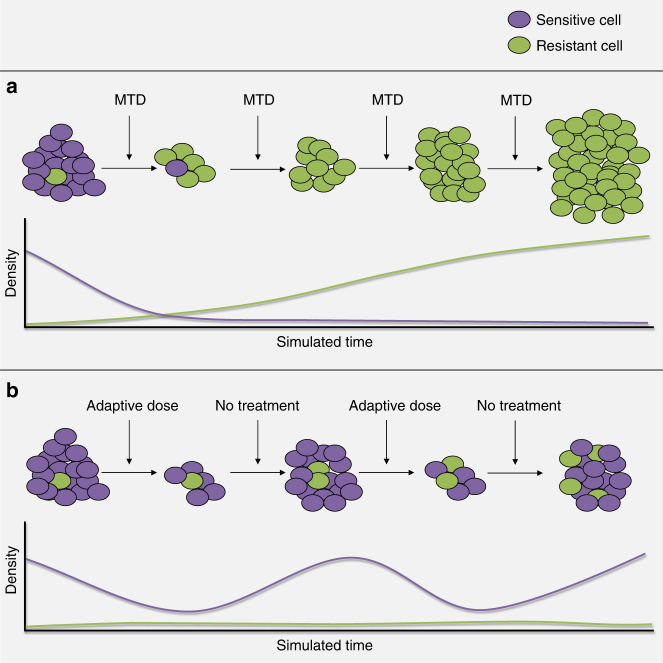
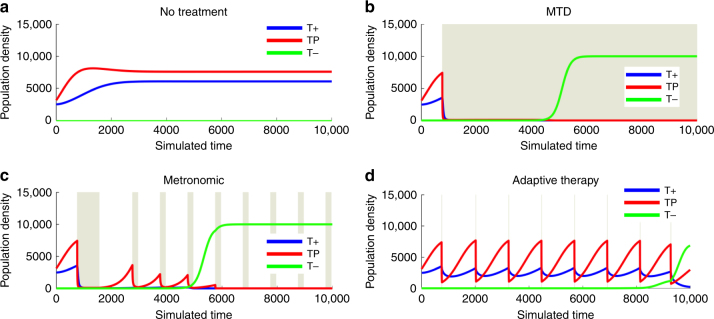
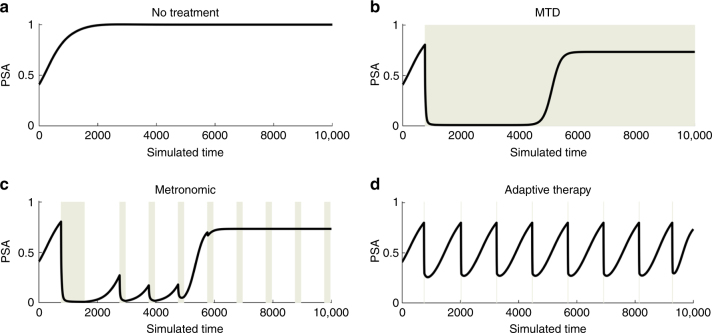
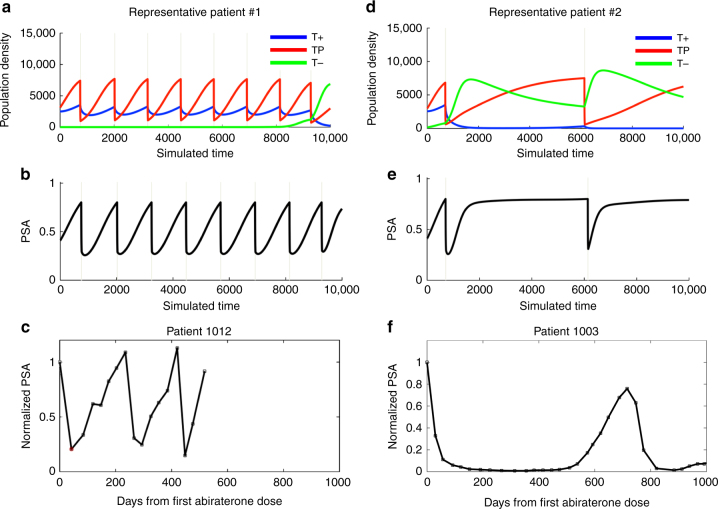
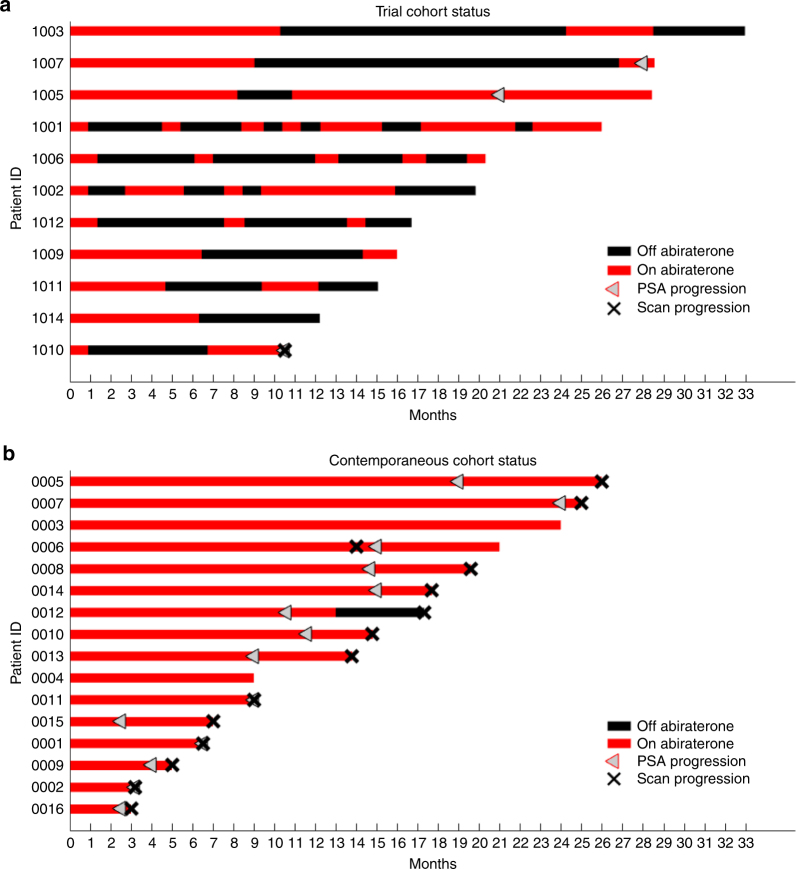
Abiraterone treats metastatic castrate-resistant prostate cancer by inhibiting CYP17A, an enzyme for testosterone auto-production. With standard dosing, evolution of resistance with treatment failure (radiographic progression) occurs at a median of ~16.5 months. We hypothesize time to progression (TTP) could be increased by integrating evolutionary dynamics into therapy. We developed an evolutionary game theory model using Lotka-Volterra equations with three competing cancer "species": androgen dependent, androgen producing, and androgen independent. Simulations with standard abiraterone dosing demonstrate strong selection for androgen-independent cells and rapid treatment failure. Adaptive therapy, using patient-specific tumor dynamics to inform on/off treatment cycles, suppresses proliferation of androgen-independent cells and lowers cumulative drug dose. In a pilot clinical trial, 10 of 11 patients maintained stable oscillations of tumor burdens; median TTP is at least 27 months with reduced cumulative drug use of 47% of standard dosing. The outcomes show significant improvement over published studies and a contemporaneous population.
Trial registration: ClinicalTrials.gov NCT02415621.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
Comment in
-
On the reporting and analysis of a cancer evolutionary adaptive dosing trial.Nat Commun. 2021 Jan 12;12(1):316. doi: 10.1038/s41467-020-20174-4. Nat Commun. 2021. PMID: 33436546 Free PMC article. No abstract available.
-
Response to Mistry.Nat Commun. 2021 Jan 12;12(1):329. doi: 10.1038/s41467-020-20175-3. Nat Commun. 2021. PMID: 33436553 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
