

Clinical outcomes of endoscope-assisted vitrectomy for treatment of rhegmatogenous retinal detachment
- PMID: 29180845
- PMCID: PMC5694206
- DOI: 10.2147/OPTH.S147690
Clinical outcomes of endoscope-assisted vitrectomy for treatment of rhegmatogenous retinal detachment
Abstract
Summary: We evaluated the clinical outcomes for ophthalmic endoscope-assisted vitrectomy in consecutive patients with uncomplicated rhegmatogenous retinal detachment (RRD). The primary success rate was 98.4% (125/127) without performing a posterior drainage retinotomy or using perfluorocarbon liquids (PFCL) for subretinal fluid drainage.
Purpose: To investigate the clinical outcomes of endoscope-assisted vitrectomy in patients with uncomplicated RRD.
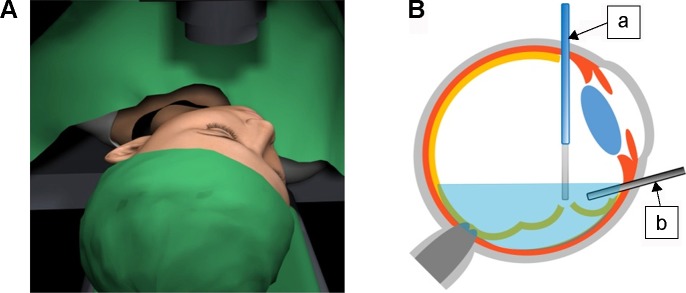
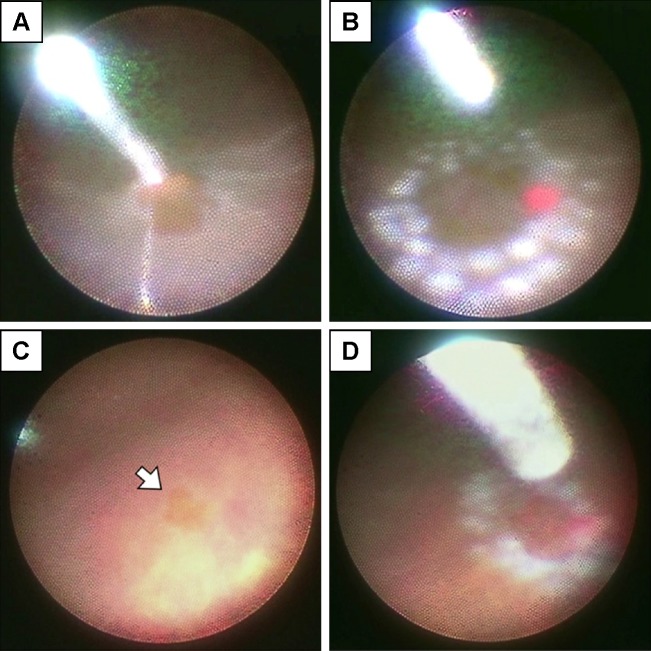
Methods: We examined 127 eyes from consecutive patients who underwent repair of RRD by 23- or 25-gauge endoscope-assisted vitrectomy, with a minimum follow-up of 3 months. Eyes with the following criteria were excluded: Giant retinal tears, grade C proliferative vitreoretinopathy, dense vitreous hemorrhage, retinal detachment secondary to other ocular diseases, and prior retinal or vitreous surgery. All cases underwent subretinal fluid drainage, endolaser photocoagulation and fundus inspection were performed under ophthalmic endoscopic observation. Success rate, visual acuity, surgery time and complications were evaluated.
Results: Primary and final success rate was 98.4% (125/127) and 100% (127/127), respectively, Surgery time was 59.6±26.3 minutes. The best-corrected visual acuity significantly improved from 20/100 to 20/20 (P<0.0001). There were 2 cases (1.6%) of creation of a peripheral drainage retinotomy and 4 cases (3.1%) of using PFCL to suppress movement of the detached retina, but there were no cases of creation of a posterior drainage retinotomy or using PFCL for subretinal fluid drainage. There was 1 case of presumed endophthalmitis after surgery. There were 12 hypotonous cases at postoperative day 1 and one of them needed additional scleral sutures at postoperative day 4 for prolonged hypotony.
Conclusion: The present study demonstrated the efficacy of endoscope-assisted vitrectomy for patients with uncomplicated RRD. To perform endoscope-assisted vitrectomy safely, sufficient closure of sclerotomies is necessary at the end of surgery.
Keywords: endoscope-assisted vitrectomy; endoscopic vitrectomy; ophthalmic endoscope; retinal detachment; rhegmatogenous retinal detachment.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Mitry D, Charteris DG, Yorston D, et al. Scottish RD Study Group The epidemiology and socioeconomic associations of retinal detachment in Scotland: a two-year prospective population-based study. Invest Ophthalmol Vis Sci. 2010;51(10):4963–4968. - PubMed
-
- Wong CW, Wong WL, Yeo IY, et al. Trends and factors related to outcomes for primary rhegmatogenous retinal detachment surgery in a large asian tertiary eye center. Retina. 2014;34(4):684–692. - PubMed
-
- Ho JD, Liou SW, Tsai CY, Tsai RJ, Lin HC. Trends and outcomes of treatment for primary rhegmatogenous retinal detachment: a 9-year nationwide population-based study. Eye (Lond) 2009;23(3):669–675. - PubMed
-
- Jonas JB, Mangler B, Decker A, Schlichtenbrede FC. Ratio of primary episcleral buckling surgery versus primary vitrectomy for rhegmatogenous retinal detachment. Eye Sci. 2014;29(1):53–54. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
