

Comparison of 3D Echocardiogram-Derived 3D Printed Valve Models to Molded Models for Simulated Repair of Pediatric Atrioventricular Valves
- PMID: 29181795
- PMCID: PMC5831483
- DOI: 10.1007/s00246-017-1785-4
Comparison of 3D Echocardiogram-Derived 3D Printed Valve Models to Molded Models for Simulated Repair of Pediatric Atrioventricular Valves
Abstract
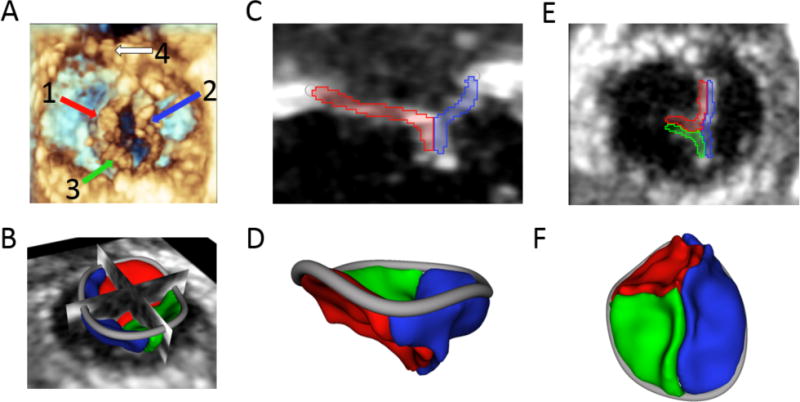
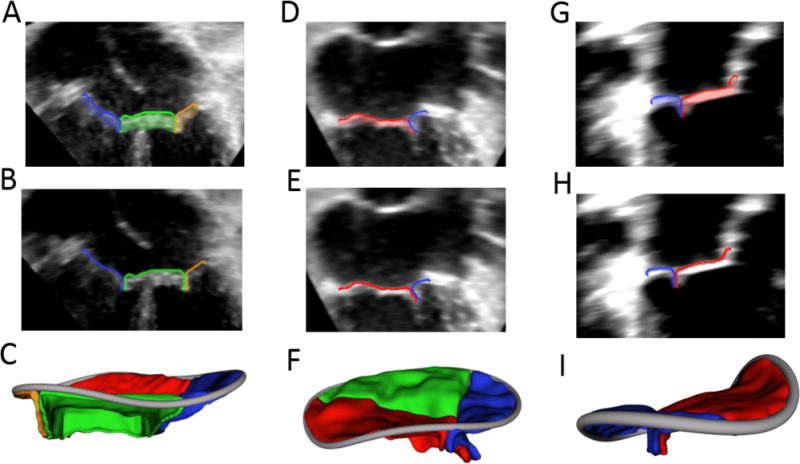
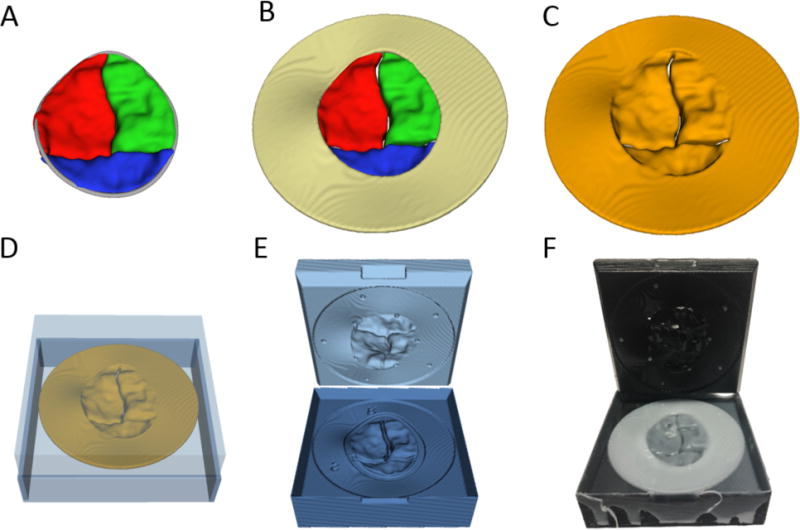
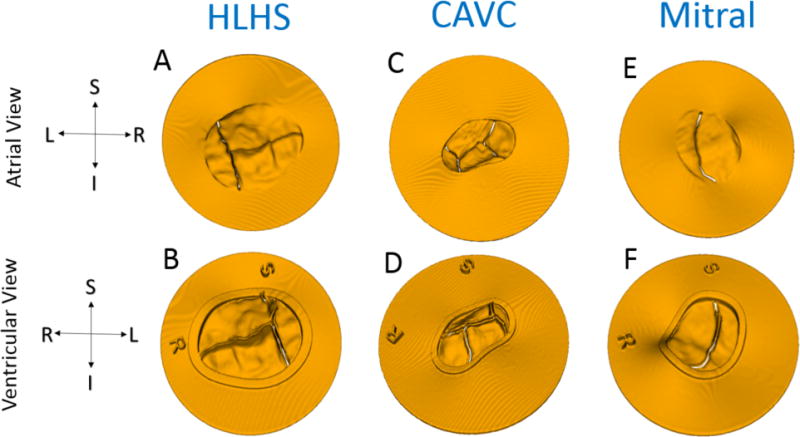
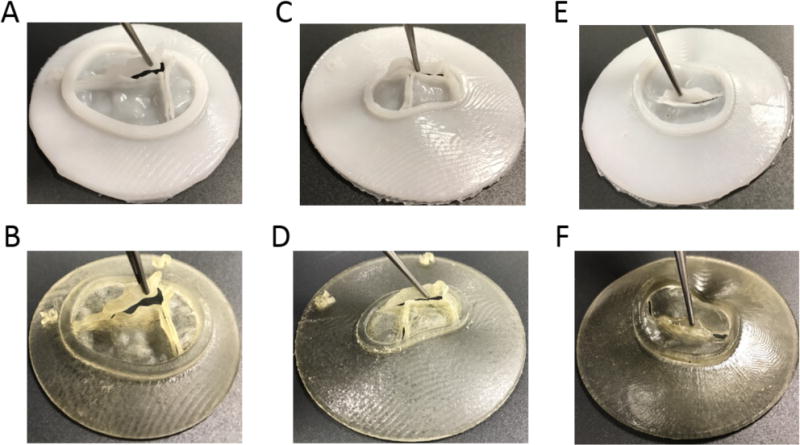
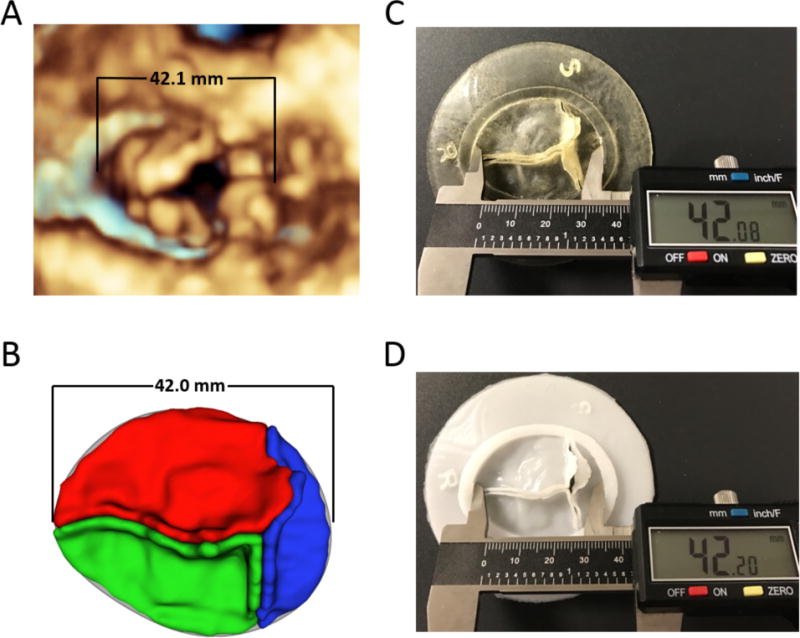
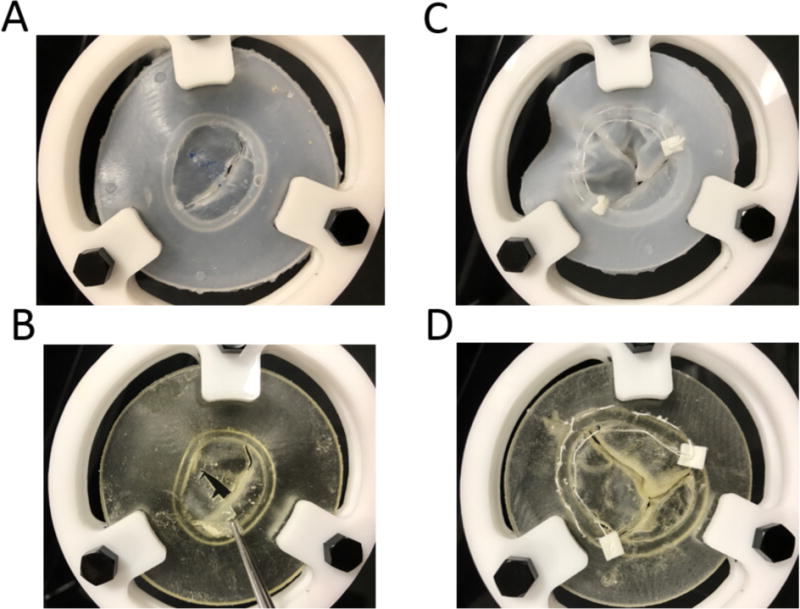
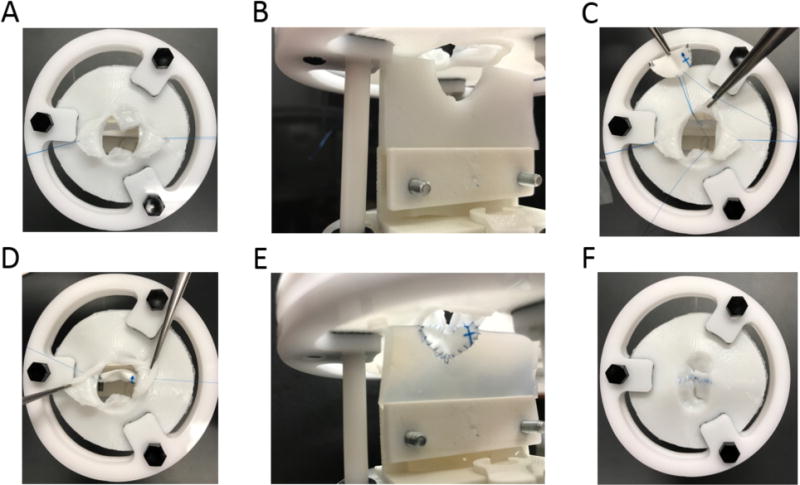
Mastering the technical skills required to perform pediatric cardiac valve surgery is challenging in part due to limited opportunity for practice. Transformation of 3D echocardiographic (echo) images of congenitally abnormal heart valves to realistic physical models could allow patient-specific simulation of surgical valve repair. We compared materials, processes, and costs for 3D printing and molding of patient-specific models for visualization and surgical simulation of congenitally abnormal heart valves. Pediatric atrioventricular valves (mitral, tricuspid, and common atrioventricular valve) were modeled from transthoracic 3D echo images using semi-automated methods implemented as custom modules in 3D Slicer. Valve models were then both 3D printed in soft materials and molded in silicone using 3D printed "negative" molds. Using pre-defined assessment criteria, valve models were evaluated by congenital cardiac surgeons to determine suitability for simulation. Surgeon assessment indicated that the molded valves had superior material properties for the purposes of simulation compared to directly printed valves (p < 0.01). Patient-specific, 3D echo-derived molded valves are a step toward realistic simulation of complex valve repairs but require more time and labor to create than directly printed models. Patient-specific simulation of valve repair in children using such models may be useful for surgical training and simulation of complex congenital cases.
Keywords: 3D echocardiography; 3D printing; Surgical simulation; Valve repair.
Conflict of interest statement
Figures
References
-
- Carpentier A, Chauvaud S, Mace L, Relland J, Mihaileanu S, Marino JP, Abry B, Guibourt P. A new reconstructive operation for Ebstein’s anomaly of the tricuspid valve. J Thorac Cardiovasc Surg. 1988;96(1):92–101. - PubMed
-
- Chauvaud S, Perier P, Touati G, Relland J, Kara SM, Benomar M, Carpentier A. Long-term results of valve repair in children with acquired mitral valve incompetence. Circulation. 1986;74(3 Pt 2):I104–109. - PubMed
-
- Galloway AC, Colvin SB, Baumann FG, Esposito R, Vohra R, Harty S, Freeberg R, Kronzon I, Spencer FC. Long-term results of mitral valve reconstruction with Carpentier techniques in 148 patients with mitral insufficiency. Circulation. 1988;78(3 Pt 2):I97–105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
