

A primary hepatic gastrinoma accompanied by hyperplasia of multi-nodular Brunner's glands
- PMID: 29181825
- PMCID: PMC5704026
- DOI: 10.1186/s40792-017-0392-1
A primary hepatic gastrinoma accompanied by hyperplasia of multi-nodular Brunner's glands
Abstract
Background: Primary hepatic gastrinoma causing severe ulcerogenic syndrome is extremely rare. Herein, we report a case of primary hepatic gastrinoma accompanied by hyperplasia of multi-nodular Brunner's glands in a patient who instead, preoperatively, was suspected of having multiple duodenal gastrinomas and hepatic metastasis.
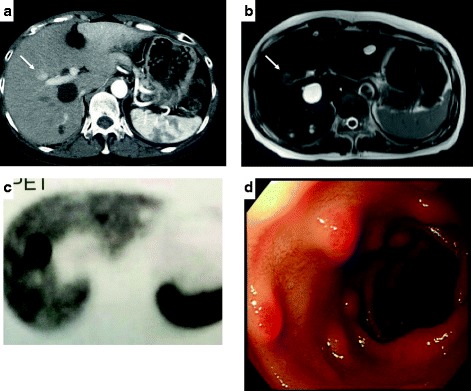
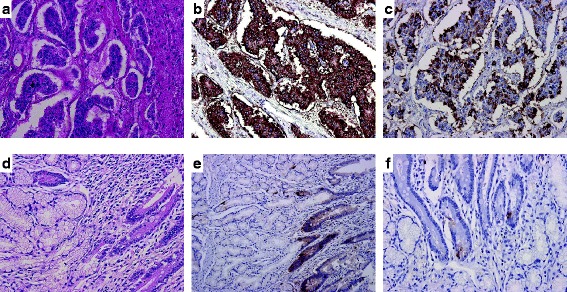
Case presentation: A 57-year-old woman consulted a clinic complaining of melena, intermittent abdominal pain, diarrhea, and vomiting which had persisted for about 3 years. Six months before her presentation, she underwent segmental resection of the jejunum for acute peritonitis due to the spontaneous jejunal perforation. A blood test revealed that her serum immunoreactive gastrin (IRG) level was 12,037 pg/mL. Subsequently, she was transferred to our hospital. On computed tomography (CT), a hypervascular tumor of 23 mm in the segment 5 (S5) region of the liver was visualized. A selective arterial secretagogue injection test (SASI test) was performed twice. The first SASI test revealed that the hepatic tumor was a gastrinoma, and there was no gastrinoma in the duodeno-pancreatic region. Additionally, somatostatin receptor scintigraphy only visualized the tumor in the liver. However, the second SASI test, which was performed during the administration of a proton pump inhibitor and a somatostatin analog (octreotide acetate), revealed that there may have been gastrinomas existing not only in the liver but also in the upper part of the duodenum or the head of the pancreas. Duodenal endoscopy revealed multiple submucosal tumors in the first and the second portion of the duodenum, although a pathological examination of biopsied specimens obtained from the duodenal lesions was negative for malignant cells. Multiple endocrine neoplasia type 1 (MEN1) was excluded from her family history, and serum levels of both intact parathyroid hormone (iPTH) and calcium were within normal ranges. An anterior segmentectomy of the liver and pancreas-preserving total duodenectomy were performed on September 9, 2013. Postoperatively, her serum immunoreactive gastrin level decreased to less than 50 pg/mL. Pathological study of the resected specimens revealed a gastrinoma in the liver, but no gastrinoma in the duodenum. Interestingly, the duodenal submucosal tumor-like lesions were hyperplastic Brunner's glands. Postoperatively, she has been well without recurrence of hypergastrinemia for 4 years.
Conclusion: We report a case of primary hepatic gastrinoma in a patient who has been cured for 4 years postoperatively. The diagnosis was somewhat difficult due to the coexisting, multiple hyperplastic Brunner's glands of the duodenum mimicking the submucosal neuroendocrine tumors, which might have developed due to long-term hypergastrinemia.
Keywords: Hypergastrinemia; Hyperplasia of Brunner’s glands; Pancreas-preserving total duodenectomy; Primary hepatic gastrinoma; Selective arterial secretagogue injection test; Somatostatin receptor scintigraphy.
Conflict of interest statement
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


Similar articles
-
Primary hepatic gastrinoma being diagnosed preoperatively: a case report and literature review.Surg Case Rep. 2020 Nov 18;6(1):290. doi: 10.1186/s40792-020-01072-9. Surg Case Rep. 2020. PMID: 33206240 Free PMC article.
-
Biochemically curative surgery for gastrinoma in multiple endocrine neoplasia type 1 patients.World J Gastroenterol. 2011 Mar 14;17(10):1343-53. doi: 10.3748/wjg.v17.i10.1343. World J Gastroenterol. 2011. PMID: 21455335 Free PMC article.
-
Gastrin Induces Nuclear Export and Proteasome Degradation of Menin in Enteric Glial Cells.Gastroenterology. 2017 Dec;153(6):1555-1567.e15. doi: 10.1053/j.gastro.2017.08.038. Epub 2017 Aug 30. Gastroenterology. 2017. PMID: 28859856 Free PMC article.
-
Novel association of duodenal gastrinoma and atrophic gastritis: case report and literature review.Endocr Pract. 2007 Nov-Dec;13(7):770-5. doi: 10.4158/EP.13.7.770. Endocr Pract. 2007. PMID: 18194935 Review.
-
Brunner's gland adenoma of duodenum: report of two cases.Int J Clin Exp Pathol. 2015 Jun 1;8(6):7565-9. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26261670 Free PMC article. Review.
Cited by
-
Primary hepatic gastrinoma being diagnosed preoperatively: a case report and literature review.Surg Case Rep. 2020 Nov 18;6(1):290. doi: 10.1186/s40792-020-01072-9. Surg Case Rep. 2020. PMID: 33206240 Free PMC article.
References
-
- Jensen RT. Zollinger-Ellison syndrome. In: Doherty GM, Skogseid B, editors. Surgical endocrinology. Philadelphia, Pittsburg: Lippincott, Williams & Wilkins; 2001. pp. 291–344.
LinkOut - more resources
Full Text Sources
Other Literature Sources
