

Epidural therapy for the treatment of severe pre-eclampsia in non labouring women
- PMID: 29181841
- PMCID: PMC6486199
- DOI: 10.1002/14651858.CD009540.pub2
Epidural therapy for the treatment of severe pre-eclampsia in non labouring women
Abstract
Background: Pre-eclampsia is a pregnancy-specific multi-organ disorder, which is characterised by hypertension and multisystem organ involvement and which has significant maternal and fetal morbidity and mortality. Failure of the placental vascular remodelling and reduced uteroplacental flow form the etiopathological basis of pre-eclampsia. There are several established therapies for pre-eclampsia including antihypertensives and anticonvulsants. Most of these therapies aim at controlling the blood pressure or preventing complications of elevated blood pressure, or both. Epidural therapy aims at blocking the vasomotor tone of the arteries, thereby increasing uteroplacental blood flow. This review was aimed at evaluating the available evidence about the possible benefits and risks of epidural therapy in the management of severe pre-eclampsia, to define the current evidence level of this therapy, and to determine what (if any) further evidence is required.
Objectives: To assess the effectiveness, safety and cost of the extended use of epidural therapy for treating severe pre-eclampsia in non-labouring women. This review aims to compare the use of extended epidural therapy with other methods, which include intravenous magnesium sulphate, anticonvulsants other than magnesium sulphate, with or without use of the antihypertensive drugs and adjuncts in the treatment of severe pre-eclampsia.This review only considered the use of epidural anaesthesia in the management of severe pre-eclampsia in the antepartum period and not as pain relief in labour.
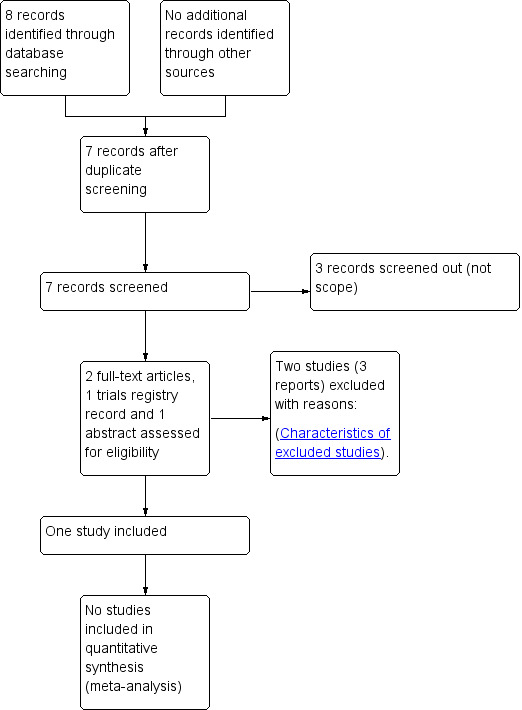
Search methods: We searched Cochrane Pregnancy and Childbirth's Trials Register, ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform (ICTRP) (13 July 2017) and reference lists of retrieved studies.
Selection criteria: Randomised controlled trials (RCTs) or quasi-RCTs comparing epidural therapy versus traditional therapy for pre-eclampsia in the form of antihypertensives, anticonvulsants, magnesium sulphate, low-dose dopamine, corticosteroids or a combination of these, were eligible for inclusion. Trials using a cluster design, and studies published in abstract form only are also eligible for inclusion in this review. Cross-over trials were not eligible for inclusion in this review.
Data collection and analysis: The two review authors independently assessed trials for inclusion and trial quality. There were no relevant data available for extraction.
Main results: We included one small study (involving 24 women). The study was a single-centre randomised trial conducted in Mexico. This study compared a control group who received antihypertensive therapy, anticonvulsant therapy, plasma expanders, corticosteroids and dypyridamole with an intervention group that received epidural block instead of the antihypertensives, as well as all the other four drugs. Lumbar epidural block was given using 0.25% bupivacaine, 10 mg bolus and 5 mg each hour on continuous epidural infusion for six hours. This study was at low risk of bias in three domains but was assessed to be high risk of bias in two domains due to lack of allocation concealment and blinding of women and staff, and unclear for random sequence generation and outcome assessor blinding.The included study did not report on any of this review's important outcomes. Meta-analysis was not possible.For the mother, these were: maternal death (death during pregnancy or up to 42 days after the end of the pregnancy, or death more than 42 days after the end of the pregnancy); development of eclampsia or recurrence of seizures; stroke; any serious morbidity: defined as at least one of stroke, kidney failure, liver failure, HELLP syndrome (haemolysis, elevated liver enzymes and low platelets), disseminated intravascular coagulation, pulmonary oedema.For the baby, these were: death: stillbirths (death in utero at or after 20 weeks' gestation), perinatal deaths (stillbirths plus deaths in the first week of life), death before discharge from the hospital, neonatal deaths (death within the first 28 days after birth), deaths after the first 28 days; preterm birth (defined as the birth before 37 completed weeks' gestation); and side effects of the intervention. Reported outcomesThe included study only reported on a single secondary outcome of interest to this review: the Apgar score of the baby at birth and after five minutes and there was no clear difference between the intervention and control groups.The included study also reported a reduction in maternal diastolic arterial pressure. However, the change in maternal mean arterial pressure and systolic arterial pressure, which were the other reported outcomes of this trial, were not significantly different between the two groups.
Authors' conclusions: Currently, there is insufficient evidence from randomised controlled trials to evaluate the effectiveness, safety or cost of using epidural therapy for treating severe pre-eclampsia in non-labouring women.High-quality randomised controlled trials are needed to evaluate the use of epidural agents as therapy for treatment of severe pre-eclampsia. The rationale for the use of epidural is well-founded. However there is insufficient evidence from randomised controlled trials to show that the effect of epidural translates into improved maternal and fetal outcomes. Thus, there is a need for larger, well-designed studies to come to an evidence-based conclusion as to whether the lowering of vasomotor tone by epidural therapy results in better maternal and fetal outcomes and for how long that could be maintained. Another important question that needs to be answered is how long should extended epidural be used to ensure any potential clinical benefits and what could be the associated side effects and costs. Interactions with other modalities of treatment and women's satisfaction could represent other avenues of research.
Conflict of interest statement
Dr Amita Ray: none known.
Dr Sujoy Ray: none known.
Figures

Update of
- doi: 10.1002/14651858.CD009540
Similar articles
-
Calcium supplementation commencing before or early in pregnancy, or food fortification with calcium, for preventing hypertensive disorders of pregnancy.Cochrane Database Syst Rev. 2017 Sep 26;9(9):CD011192. doi: 10.1002/14651858.CD011192.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2019 Sep 16;9:CD011192. doi: 10.1002/14651858.CD011192.pub3. PMID: 28949421 Free PMC article. Updated.
-
Use of biochemical tests of placental function for improving pregnancy outcome.Cochrane Database Syst Rev. 2015 Nov 25;2015(11):CD011202. doi: 10.1002/14651858.CD011202.pub2. Cochrane Database Syst Rev. 2015. PMID: 26602956 Free PMC article.
-
Amnioinfusion for chorioamnionitis.Cochrane Database Syst Rev. 2016 Aug 24;2016(8):CD011622. doi: 10.1002/14651858.CD011622.pub2. Cochrane Database Syst Rev. 2016. PMID: 27556818 Free PMC article.
-
Epidural versus non-epidural or no analgesia for pain management in labour.Cochrane Database Syst Rev. 2018 May 21;5(5):CD000331. doi: 10.1002/14651858.CD000331.pub4. Cochrane Database Syst Rev. 2018. PMID: 29781504 Free PMC article.
-
Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour.Cochrane Database Syst Rev. 2015 Dec 14;2015(12):CD011200. doi: 10.1002/14651858.CD011200.pub2. Cochrane Database Syst Rev. 2015. PMID: 26662716 Free PMC article.
Cited by
-
Clinical Effects of Integrated Traditional Chinese and Western Medicine in Treating Severe Preeclampsia and Its Influence on Maternal and Infant Outcomes after Cesarean Section under Combined Lumbar and Epidural Anesthesia.Evid Based Complement Alternat Med. 2021 Nov 8;2021:6366914. doi: 10.1155/2021/6366914. eCollection 2021. Evid Based Complement Alternat Med. 2021. PMID: 34790247 Free PMC article.
-
Association of epidural labor analgesia with maternal and neonatal outcomes in women with preeclampsia: a propensity score-matched single-center retrospective cohort study.BMC Pregnancy Childbirth. 2025 Jan 24;25(1):66. doi: 10.1186/s12884-025-07155-5. BMC Pregnancy Childbirth. 2025. PMID: 39856582 Free PMC article.
References
References to studies included in this review
Pardo Morales 2004 {published data only}
-
- Pardo‐Morales RV, Romero‐Figueroa S, Vazquez‐de Anda GF, Briones‐Garduno JC, Herrera‐Villalobos JE, Gonzalez‐Vargas A. A new therapeutic approach to severe preeclampsia. Cirugia y Cirujanos 2004;72(3):203‐7. - PubMed
References to studies excluded from this review
Ginosar 2009 {published data only}
-
- Ginosar Y, Nadjari M, Hoffman A, Firman N, Davidson EM, Weiniger CF, et al. Antepartum continuous epidural ropivacaine therapy reduces uterine artery vascular resistance in pre‐eclampsia: a randomised, dose‐ranging, placebo‐controlled study. British Journal of Anaesthesia 2009;102(3):369‐78. - PubMed
-
- NCT00197340. Antepartum chronic epidural therapy (ACET) to improve blood flow to the uterus, placenta and baby in pre‐eclampsia and intrauterine growth restriction. clinicaltrials.gov/show/NCT00197340 Date first received: 13 September 2005.
Pyregov 2010 {published data only}
-
- Pyregov A, Shifman E, Sukhih G. How ropivacaine epidural infusion influences on some plasma cytokines concentration in pregnant women with severe preeclampsia?. Regional Anesthesia and Pain Medicine 2010;35(5):E157.
Additional references
Abalos 2014
Ahmed 2004
-
- Ahmad S, Ahmed A. Elevated placental soluble vascular endothelial growth factor receptor‐1inhibits angiogenesis in preeclampsia. Circulation Research 2004;95:884‐91. - PubMed
Bergel 2002
Brown 2000
-
- Brown MA, Hague WM, Higgins J, Lowe S, McCowan L, Oats J, et al. The detection, investigation and management of hypertension in pregnancy: full consensus statement. Australian and New Zealand Journal of Obstetrics and Gynaecology 2000;40(2):139‐55. - PubMed
CEMACH 2007
-
- Lewis G (editor). The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers' Lives: reviewing maternal deaths to make motherhood safer ‐ 2003‐2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. http://www.mdeireland.com/pub/SML07_Report.pdf (accessed 10 October 2011) 2007.
Churchill 2007
Cruickshank 1992
-
- Cruickshank DJ, Robertson AA, Campbell DM, MacGillivray I. Does labetalol influence the development of proteinuria in pregnancy hypertension? A randomised controlled study. European Journal of Obstetrics & Gynecology and Reproductive Biology 1992;45(1):47‐51. [PUBMED: 1618361] - PubMed
Cunningham 2014
-
- Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe J. Williams Obstetrics. McGraw Hill, 2014.
Dowswell 2009
Dowswell 2015
Duley 2005
Duley 2009
-
- Duley L, Henderson‐Smart DJ, Walker GJA. Interventions for treating pre‐eclampsia and its consequences: generic protocol. Cochrane Database of Systematic Reviews 2009, Issue 2. [DOI: 10.1002/14651858.CD007756] - DOI
Duley 2010a
Duley 2010b
Duley 2010c
Duley 2010d
Duley 2010e
Gabbe 2013
-
- Gabbe SG, Landon MB, Niebyl JR, Galan HL, Simpson JL, Jauniax ERM, et al. Obstetrics : Normal and Problem Pregnancies. Elsevier, 2013.
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hofmeyr 2014
Kanayama 1999
-
- Kanayama N, Belayet HM, Khatun S, Tokunaga N, Sugimura M, Kobayashi T, et al. A new treatment of severe pre‐eclampsia by long‐term epidural anaesthesia. Journal of Human Hypertension 1999;13(3):167‐71. [PUBMED: 10204812] - PubMed
Leighton 2002
-
- Leighton BL, Halpern SH. The effects of epidural analgesia on labor,maternal, and neonatal outcomes: A systematic review. American Journal of Obstetrics and Gynecology 2002;186:S69‐S77. - PubMed
Magpie 2002
-
- Altman D, Carroli G, Duley L, Farrell B, Moodley J, Neilson J, et al. Do women with pre‐eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo‐controlled trial. Lancet 2002; Vol. 359, issue 9321:1877‐90. - PubMed
Makrides 2006
Makrides 2014
Malvasi 2009
-
- Malvasi A, Tinelli A, Brizzi A, Greco F, Celleno D, Tinelli R. Long‐term epidural analgesia treatment in pre‐eclamptic women: a preliminary trial. Journal of Obstetrics and Gynaecology 2009;29(2):114‐8. [PUBMED: 19274543] - PubMed
Maynard 2003
Maynard 2011
Meher 2006a
Meher 2006b
Meher 2006c
Meher 2006d
Meher 2007
Nelson Piercy 2007
-
- Nelson Piercy C. Handbook of Obstetric Medicine. 3rd Edition. London: Informa Healthcare, 2007.
NHBPEP 2000
-
- Anonymous. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. American Journal of Obstetrics and Gynecology 2000;183(1):S1‐S22. - PubMed
Ota 2015a
Ota 2015b
Rana 2007
-
- Rana S, Karumanchi SA, Levine RJ, Venkatesha S, Rauh‐Hain JA, Tamez H, et al. Sequential changes in antiangiogenic factors in early pregnancy and risk of developing preeclampsia. Hypertension 2007;50( 1 ):137‐72. - PubMed
RCOG 2006
-
- Royal College of Obstetricians and Gynaecologists. Severe Pre‐eclampsia/Eclampsia, Management (Green‐top guideline 10A). London: RCOG, 2006.
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rumbold 2008
Sharrrock 1996
-
- Sharrock NE, Salvati EA. Hypotensive epidural anesthesia for total hip arthroplasty: a review. Acta Orthopaedica Scandinavica 1996;61(1):91‐107. - PubMed
Simmons 2012
Steyn 2007
Walker 2003
WHO 1988
-
- World Health Organization. Geographic variation in the incidence of hypertension in pregnancy. World Health Organization International Collaborative Study of Hypertensive Disorders of Pregnancy. American Journal of Obstetrics and Gynecology 1988;158(1):80‐3. - PubMed
WHO 2005
-
- World Health Organization. The World Health Report 2005: Make Every Mother and Child Count. Geneva: WHO, 2005.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources