

Treatment eligibility and retention in clinical HIV care: A regression discontinuity study in South Africa
- PMID: 29182641
- PMCID: PMC5705070
- DOI: 10.1371/journal.pmed.1002463
Treatment eligibility and retention in clinical HIV care: A regression discontinuity study in South Africa
Abstract
Background: Loss to follow-up is high among HIV patients not yet receiving antiretroviral therapy (ART). Clinical trials have demonstrated the clinical efficacy of early ART; however, these trials may miss an important real-world consequence of providing ART at diagnosis: its impact on retention in care.
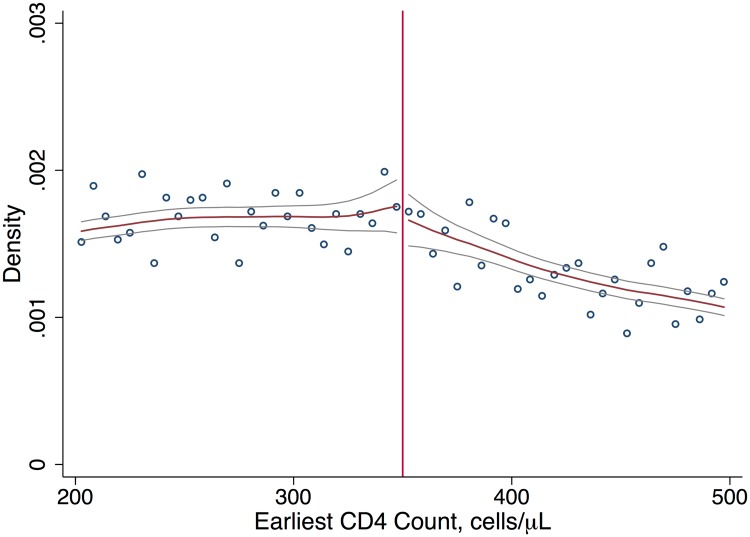
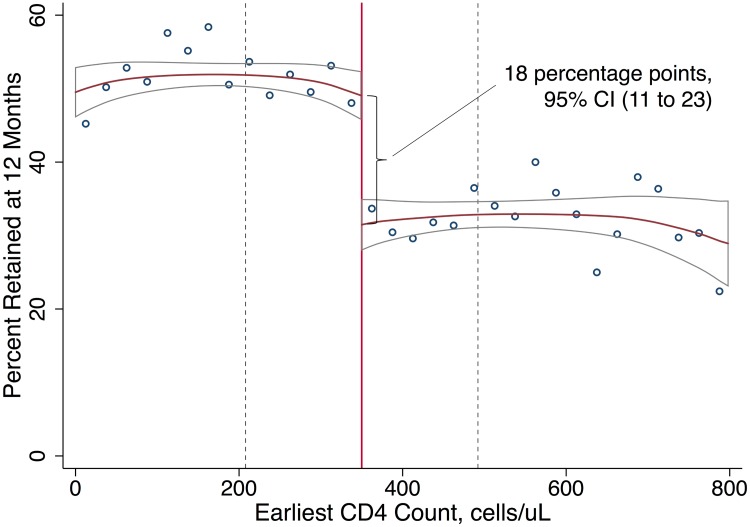
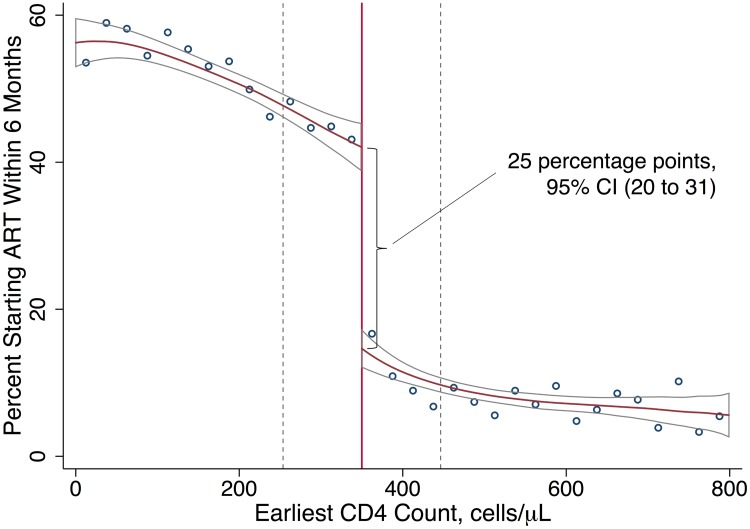
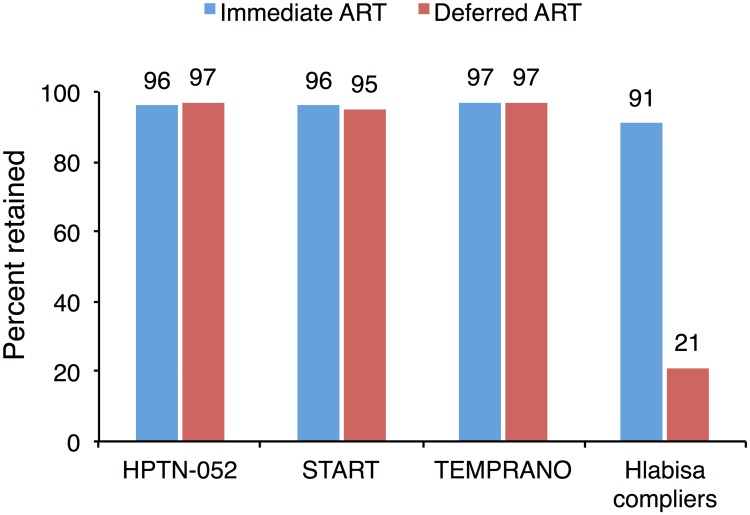
Methods and findings: We examined the effect of immediate (versus deferred) ART on retention in care using a regression discontinuity design. The analysis included all patients (N = 11,306) entering clinical HIV care with a first CD4 count between 12 August 2011 and 31 December 2012 in a public-sector HIV care and treatment program in rural South Africa. Patients were assigned to immediate versus deferred ART eligibility, as determined by a CD4 count < 350 cells/μl, per South African national guidelines. Patients referred to pre-ART care were instructed to return every 6 months for CD4 monitoring. Patients initiated on ART were instructed to return at 6 and 12 months post-initiation and annually thereafter for CD4 and viral load monitoring. We assessed retention in HIV care at 12 months, as measured by the presence of a clinic visit, lab test, or ART initiation 6 to 18 months after initial CD4 test. Differences in retention between patients presenting with CD4 counts just above versus just below the 350-cells/μl threshold were estimated using local linear regression models with a data-driven bandwidth and with the algorithm for selecting the bandwidth chosen ex ante. Among patients with CD4 counts close to the 350-cells/μl threshold, having an ART-eligible CD4 count (<350 cells/μl) was associated with higher 12-month retention than not having an ART-eligible CD4 count (50% versus 32%), an intention-to-treat risk difference of 18 percentage points (95% CI 11 to 23; p < 0.001). The decision to start ART was determined by CD4 count for one in four patients (25%) presenting close to the eligibility threshold (95% CI 20% to 31%; p < 0.001). In this subpopulation, having an ART-eligible CD4 count was associated with higher 12-month retention than not having an ART-eligible CD4 count (91% versus 21%), a complier causal risk difference of 70 percentage points (95% CI 42 to 98; p < 0.001). The major limitations of the study are the potential for limited generalizability, the potential for outcome misclassification, and the absence of data on longer-term health outcomes.
Conclusions: Patients who were eligible for immediate ART had dramatically higher retention in HIV care than patients who just missed the CD4-count eligibility cutoff. The clinical and population health benefits of offering immediate ART regardless of CD4 count may be larger than suggested by clinical trials.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: SR is a member of the Editorial Board of PLOS Medicine.
Figures
References
-
- Bor J, Herbst A, Newell M-L, Bärnighausen T. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment. Science. 2013;339:961–5. doi: 10.1126/science.1230413 - DOI - PMC - PubMed
-
- Mills EJ, Bakanda C, Birungi J, Chan K, Ford N, Cooper CL, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Ann Intern Med. 2011;155:209–17. doi: 10.7326/0003-4819-155-4-201108160-00358 - DOI - PubMed
-
- Bendavid E, Holmes CB, Bhattacharya J, Miller G. HIV development assistance and adult mortality in Africa. JAMA. 2012;307:2060–7. doi: 10.1001/jama.2012.2001 - DOI - PMC - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–128. doi: 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- Grinsztejn B, Hosseinipour MC, Ribaudo HJ, Swindells S, Eron J, Chen YQ, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis. 2014;14:281–90. doi: 10.1016/S1473-3099(13)70692-3 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
