

Association Between Wait Time and 30-Day Mortality in Adults Undergoing Hip Fracture Surgery
- PMID: 29183076
- PMCID: PMC5820694
- DOI: 10.1001/jama.2017.17606
Association Between Wait Time and 30-Day Mortality in Adults Undergoing Hip Fracture Surgery
Abstract
Importance: Although wait times for hip fracture surgery have been linked to mortality and are being used as quality-of-care indicators worldwide, controversy exists about the duration of the wait that leads to complications.
Objective: To use population-based wait-time data to identify the optimal time window in which to conduct hip fracture surgery before the risk of complications increases.
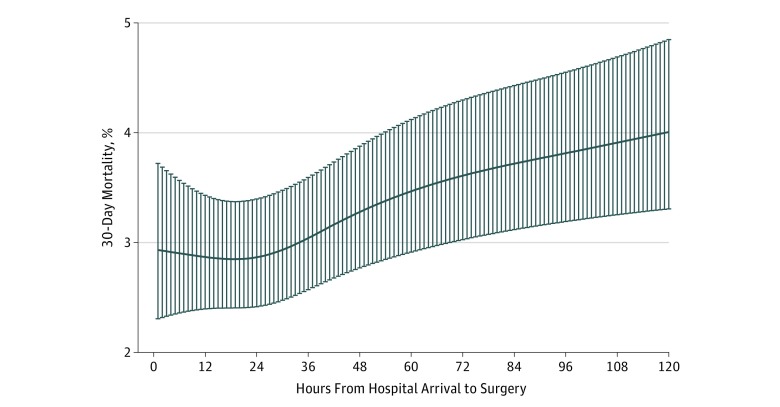
Design, setting, and participants: Population-based, retrospective cohort study of adults undergoing hip fracture surgery between April 1, 2009, and March 31, 2014, at 72 hospitals in Ontario, Canada. Risk-adjusted restricted cubic splines modeled the probability of each complication according to wait time. The inflection point (in hours) when complications began to increase was used to define early and delayed surgery. To evaluate the robustness of this definition, outcomes among propensity-score matched early and delayed surgical patients were compared using percent absolute risk differences (RDs, with 95% CIs).
Exposure: Time elapsed from hospital arrival to surgery (in hours).
Main outcomes and measures: Mortality within 30 days. Secondary outcomes included a composite of mortality or other medical complications (myocardial infarction, deep vein thrombosis, pulmonary embolism, and pneumonia).
Results: Among 42 230 patients with hip fracture (mean [SD] age, 80.1 years [10.7], 70.5% women) who met study entry criteria, overall mortality at 30 days was 7.0%. The risk of complications increased when wait times were greater than 24 hours, irrespective of the complication considered. Compared with 13 731 propensity-score matched patients who received surgery earlier, 13 731 patients who received surgery after 24 hours had a significantly higher risk of 30-day mortality (898 [6.5%] vs 790 [5.8%]; % absolute RD, 0.79; 95% CI, 0.23-1.35) and the composite outcome (1680 [12.2%]) vs 1383 [10.1%]; % absolute RD, 2.16; 95% CI, 1.43-2.89).
Conclusions and relevance: Among adults undergoing hip fracture surgery, increased wait time was associated with a greater risk of 30-day mortality and other complications. A wait time of 24 hours may represent a threshold defining higher risk.
Conflict of interest statement
Figures

Comment in
-
Timing of Operations and Outcomes for Patients With Hip Fracture-It's Probably Not Worth the Wait.JAMA. 2017 Nov 28;318(20):1981-1982. doi: 10.1001/jama.2017.17624. JAMA. 2017. PMID: 29183051 No abstract available.
-
[Comments on: Timing of operative treatment of fractures near the hip joint].Anaesthesist. 2018 Jun;67(6):458-460. doi: 10.1007/s00101-018-0449-y. Anaesthesist. 2018. PMID: 29728710 German. No abstract available.
-
Wait Time for Hip Fracture Surgery and Mortality.JAMA. 2018 Jun 5;319(21):2233. doi: 10.1001/jama.2018.4418. JAMA. 2018. PMID: 29872850 No abstract available.
-
Wait Time for Hip Fracture Surgery and Mortality.JAMA. 2018 Jun 5;319(21):2234. doi: 10.1001/jama.2018.4422. JAMA. 2018. PMID: 29872851 No abstract available.
References
-
- Pincus D, Desai SJ, Wasserstein D, et al. Outcomes of after-hours hip fracture surgery. J Bone Joint Surg Am. 2017;99(11):914-922. - PubMed
-
- Dy CJ, McCollister KE, Lubarsky DA, Lane JM. An economic evaluation of a systems-based strategy to expedite surgical treatment of hip fractures. J Bone Joint Surg Am. 2011;93(14):1326-1334. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
