

Comparison of adiposity indicators associated with fasting-state insulinemia, triglyceridemia, and related risk biomarkers in a nationally representative, adult population
- PMID: 29183845
- PMCID: PMC6003239
- DOI: 10.1016/j.diabres.2017.11.019
Comparison of adiposity indicators associated with fasting-state insulinemia, triglyceridemia, and related risk biomarkers in a nationally representative, adult population
Abstract
Aims: We hypothesized that height-corrected abdominal size (supine sagittal abdominal diameter/height ratio [SADHtR] or waist circumference/height ratio [WHtR]) would associate more strongly than body mass index (BMI, weight/height2) with levels of fasting insulin, triglycerides, and three derived biomarkers of insulin resistance.
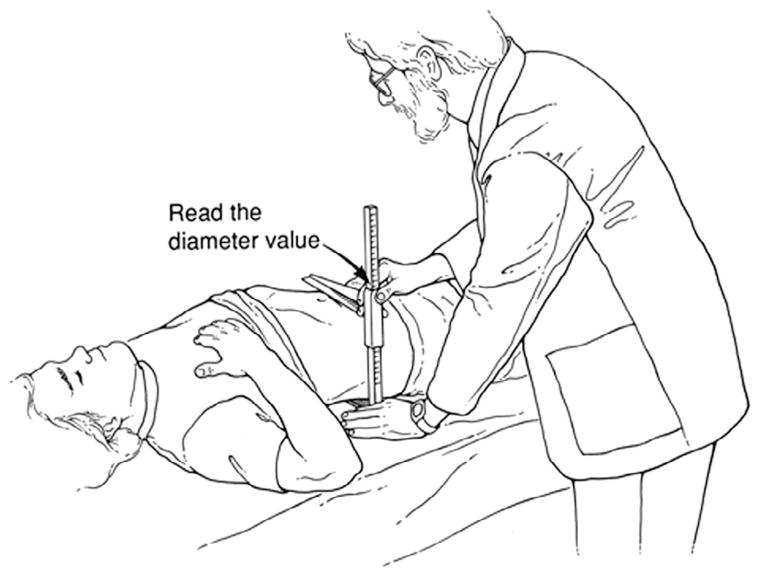
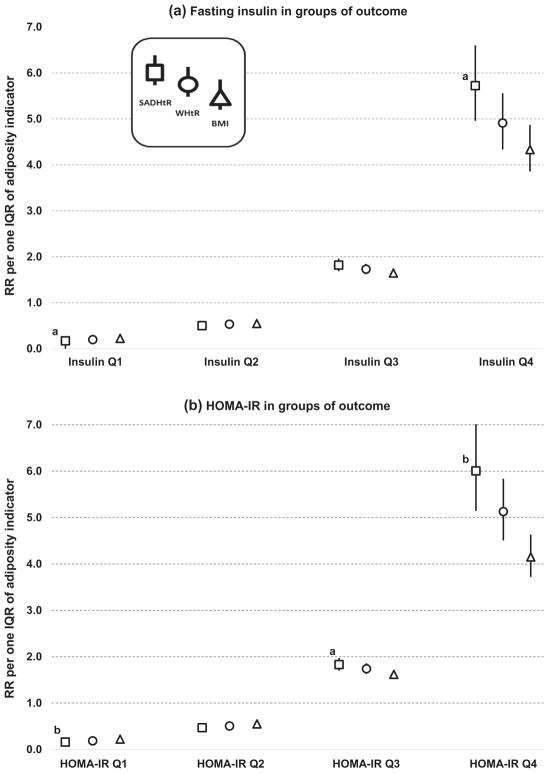
Methods: Anthropometry, including SAD by caliper, was collected on 4398 adults in the 2011-2014 National Health and Nutrition Examination Survey. For comparison purposes, each adiposity indicator was scaled to its population-based, sex-specific, interquartile range (IQR). For each biomarker we created four outcome groups based on equal-sized populations with ascending values. Multivariable polytomous logistic regression modeled the relationships between the adiposity indicators and each biomarker.
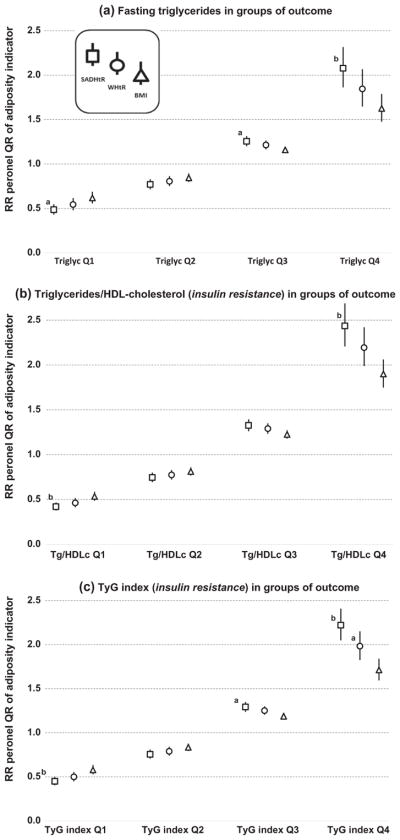
Results: Highest-group insulin was associated with a one-IQR increment of BMI (RR 4.3 [95% CI 3.9-4.9]), but more strongly with a one-IQR increment of SADHtR (RR 5.7 [5.0-6.6]). For highest-group HOMA-IR the RR for BMI (4.2 [3.7-4.6]) was less than that of SADHtR (6.0 [5.1-7.0]). Similarly, RRs for BMI were smaller than those for SADHtR applying to highest-group triglycerides (RR 1.6 vs 2.1), triglycerides/HDL-cholesterol (RR 1.9 vs 2.4) and TyG index (RR 1.7 vs 2.2) (all p < .001). The RRs for WHtR were consistently between those for SADHtR and BMI. The top 25% of insulin resistance among US adults was estimated to lie above adiposity thresholds of 0.140 for SADHtR, 0.606 for WHtR, or 29.6 kg/m2 for BMI.
Conclusions: Relative abdominal size rather than relative weight may better define adiposity associated with homeostatic insulin resistance. These population-based, cross-sectional findings could improve anthropometric prediction of cardiometabolic risk.
Keywords: Anthropometry; Body mass index; Insulin resistance; Obesity, abdominal; Sagittal abdominal diameter; Waist-height ratio.
Published by Elsevier B.V.
Conflict of interest statement
The authors declare that there is no conflict of interest associated with this manuscript.
Figures
References
-
- Bastien M, Poirier P, Lemieux I, Despres JP. Overview of epidemiology and contribution of obesity to cardiovascular disease. Prog Cardiovasc Dis. 2014;56:369–81. - PubMed
-
- Pischon T, Boeing H, Hoffmann K, Bergmann M, Schulze MB, Overvad K, et al. General and abdominal adiposity and risk of death in Europe. N Engl J Med. 2008;359:2105–20. - PubMed
-
- World Health Organization. Waist circumference and waist– hip ratio: Report of a WHO expert consultation; Geneva. 8–11 December, 2008; Geneva, Switzerland: WHO; 2011. [cited 16 October 2017]. Available from: http://apps.who.int/iris/bitstream/10665/44583/1/9789241501491_eng.pdf.
-
- Freisling H, Arnold M, Soerjomataram I, O’Doherty MG, Ordonez-Mena JM, Bamia C, et al. Comparison of general obesity and measures of body fat distribution in older adults in relation to cancer risk: meta-analysis of individual participant data of seven prospective cohorts in Europe. Br J Cancer. 2017;116:1486–97. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
