

Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis
- PMID: 29183961
- PMCID: PMC5704695
- DOI: 10.1136/bmj.j5058
Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis
Erratum in
-
Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis.BMJ. 2017 Dec 4;359:j5631. doi: 10.1136/bmj.j5631. BMJ. 2017. PMID: 29203465 No abstract available.
-
Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis.BMJ. 2018 May 23;361:k2295. doi: 10.1136/bmj.k2295. BMJ. 2018. PMID: 29793960 Free PMC article. No abstract available.
Abstract
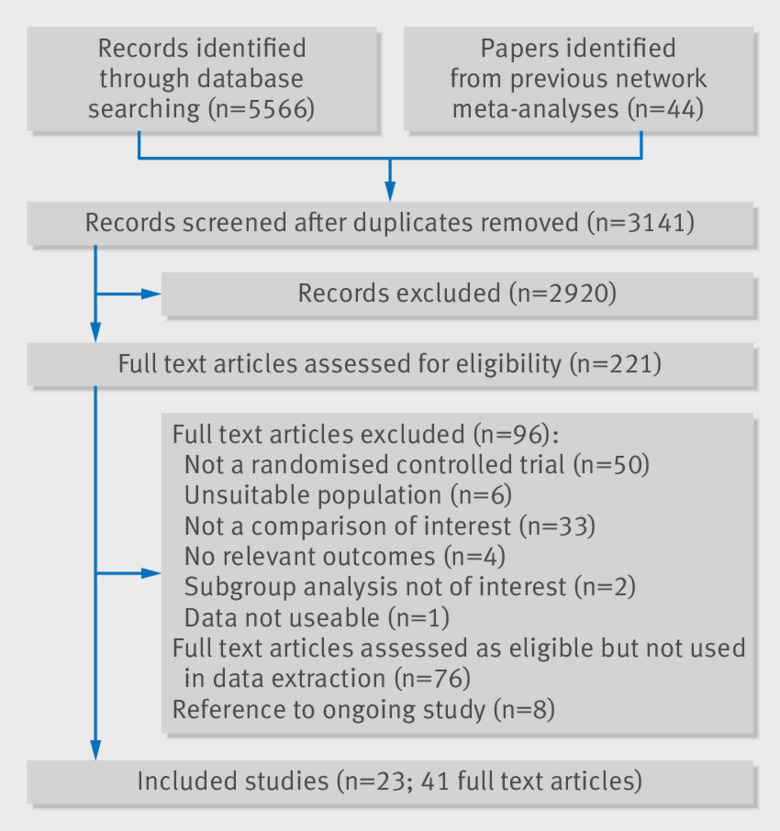
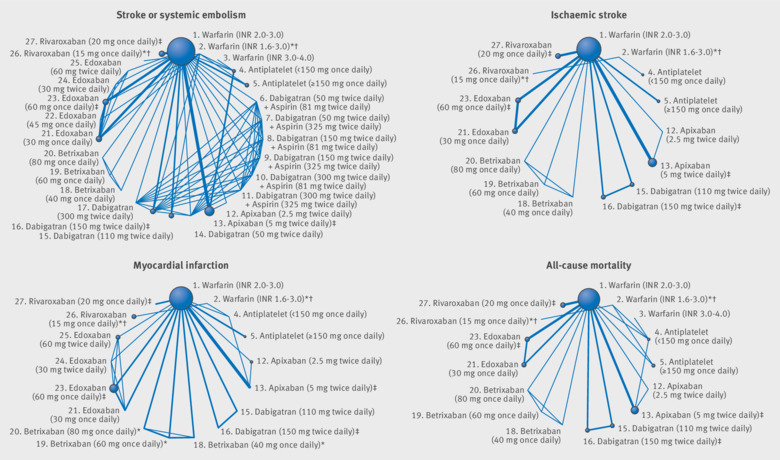
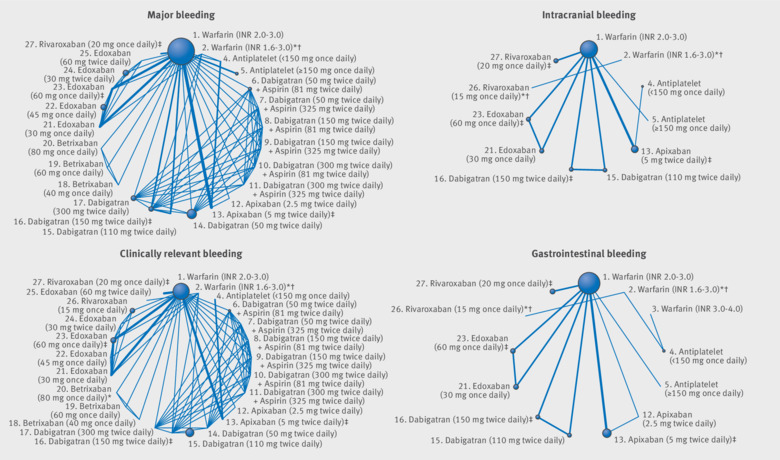
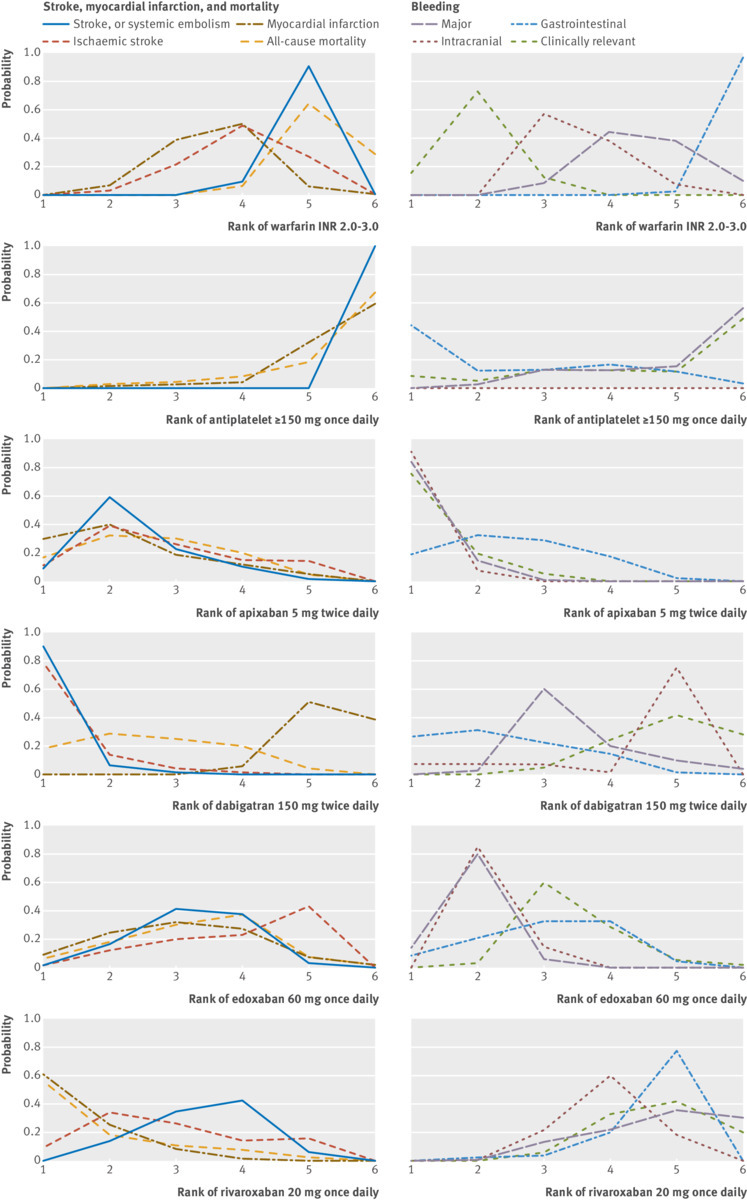
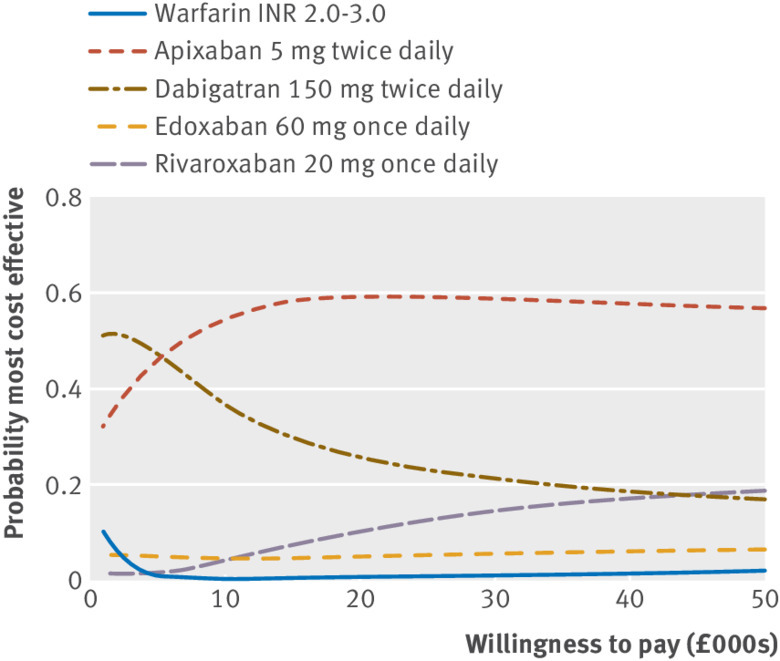
Objective To compare the efficacy, safety, and cost effectiveness of direct acting oral anticoagulants (DOACs) for patients with atrial fibrillation.Design Systematic review, network meta-analysis, and cost effectiveness analysis. Data sources Medline, PreMedline, Embase, and The Cochrane Library.Eligibility criteria for selecting studies Published randomised trials evaluating the use of a DOAC, vitamin K antagonist, or antiplatelet drug for prevention of stroke in patients with atrial fibrillation.Results 23 randomised trials involving 94 656 patients were analysed: 13 compared a DOAC with warfarin dosed to achieve a target INR of 2.0-3.0. Apixaban 5 mg twice daily (odds ratio 0.79, 95% confidence interval 0.66 to 0.94), dabigatran 150 mg twice daily (0.65, 0.52 to 0.81), edoxaban 60 mg once daily (0.86, 0.74 to 1.01), and rivaroxaban 20 mg once daily (0.88, 0.74 to 1.03) reduced the risk of stroke or systemic embolism compared with warfarin. The risk of stroke or systemic embolism was higher with edoxaban 60 mg once daily (1.33, 1.02 to 1.75) and rivaroxaban 20 mg once daily (1.35, 1.03 to 1.78) than with dabigatran 150 mg twice daily. The risk of all-cause mortality was lower with all DOACs than with warfarin. Apixaban 5 mg twice daily (0.71, 0.61 to 0.81), dabigatran 110 mg twice daily (0.80, 0.69 to 0.93), edoxaban 30 mg once daily (0.46, 0.40 to 0.54), and edoxaban 60 mg once daily (0.78, 0.69 to 0.90) reduced the risk of major bleeding compared with warfarin. The risk of major bleeding was higher with dabigatran 150 mg twice daily than apixaban 5 mg twice daily (1.33, 1.09 to 1.62), rivaroxaban 20 mg twice daily than apixaban 5 mg twice daily (1.45, 1.19 to 1.78), and rivaroxaban 20 mg twice daily than edoxaban 60 mg once daily (1.31, 1.07 to 1.59). The risk of intracranial bleeding was substantially lower for most DOACs compared with warfarin, whereas the risk of gastrointestinal bleeding was higher with some DOACs than warfarin. Apixaban 5 mg twice daily was ranked the highest for most outcomes, and was cost effective compared with warfarin.Conclusions The network meta-analysis informs the choice of DOACs for prevention of stroke in patients with atrial fibrillation. Several DOACs are of net benefit compared with warfarin. A trial directly comparing DOACs would overcome the need for indirect comparisons to be made through network meta-analysis.Systematic review registration PROSPERO CRD 42013005324.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: JACS was a former member of the Health Technology Assessment Clinical Trial Board. CS is currently a Health Services and Delivery Research - Researcher Led Board member. NJW, JS, and SD report NIHR and Medical Research Council grants during the conduct of the study, outside the present work. Other authors have no potential conflicts of interest to declare.
Figures
Comment in
-
Which anticoagulant for stroke prevention in atrial fibrillation?BMJ. 2017 Nov 28;359:j5399. doi: 10.1136/bmj.j5399. BMJ. 2017. PMID: 29183874 No abstract available.
-
Cost-effectiveness of direct acting oral anticoagulants in the prevention of thromboembolic complications: limits and concerns of economic evaluations.J Cardiovasc Med (Hagerstown). 2019 Aug;20(8):500-503. doi: 10.2459/JCM.0000000000000805. J Cardiovasc Med (Hagerstown). 2019. PMID: 31033777
References
-
- Kannel W, Wolf P, Benjamin E, et al. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: Population-based estimates. Am J Cardiol 1998;82(8A):2N-9N. - PubMed
-
- National Collaborating Centre for Chronic Conditions Atrial fibrillation: national clinical guideline for management in primary and secondary care. Royal College of Physicians, 2006. - PubMed
-
- Royal College of Physicians Sentinel Stroke National Audit Programme (SSNAP). Clinical audit April - June 2015 report prepared by Royal College of Physicians, Clinical Effectiveness and Evaluation Unit on behalf of the Intercollegiate Stroke Working Party. https://www.strokeaudit.org/Documents/National/PostAcuteOrg/2015/2015-PA...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical