

A Rare Case of Bochdalek Hernia with Concomitant Para-Esophageal Hernia, Repaired Laparoscopically in an Octogenarian
- PMID: 29184050
- PMCID: PMC5716375
- DOI: 10.12659/ajcr.906225
A Rare Case of Bochdalek Hernia with Concomitant Para-Esophageal Hernia, Repaired Laparoscopically in an Octogenarian
Abstract
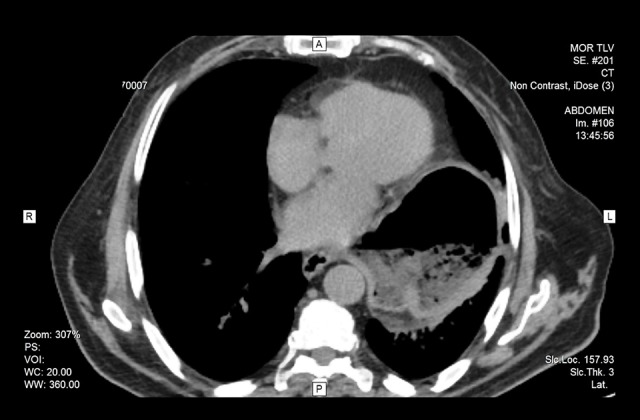
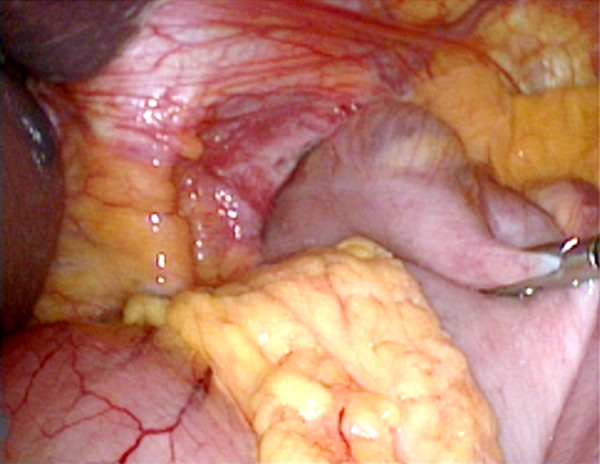
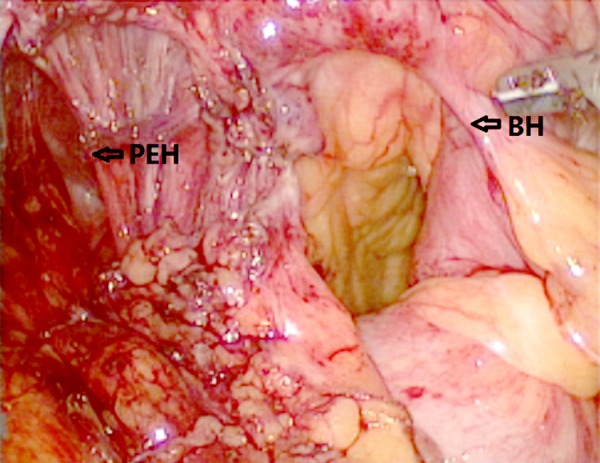
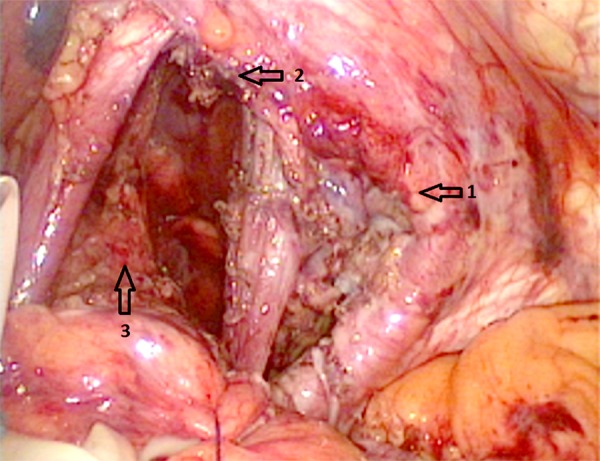
BACKGROUND A Bochdalek hernia (BH) is a rare congenital condition consisting of a posterolateral defect in the diaphragm. A para-esophageal hernia (PEH) is a rare variant of hiatus hernia. BH and PEH may present with gastric volvulus or incarceration, requiring emergency treatment. Minimally invasive surgery is the preferred treatment, particularly for elderly patients and patients with comorbidities. The occurrence of BH with concomitant PEH is a very rare event. We describe a case of an octogenarian patient with BH and concomitant PEH treated laparoscopically. CASE REPORT An 81-year-old male patient, without significant comorbidities, presented with a two-month history of severe chest pain and vomiting after eating. Cardiological investigations ruled out cardiac ischemia, infarction, or other cardiovascular abnormalities. Chest and abdominal computed tomography (CT) imaging demonstrated a large diaphragmatic hernia, with the entire stomach in the left thorax. Laboratory results showed mild anemia and a low iron level. The patient underwent simultaneous laparoscopic repair of a BH and a PEH with mesh reinforcement without antireflux fundoplication. The patient's postoperative recovery was uneventful. CONCLUSIONS We have presented a rare case of BH with concomitant PEH in an octogenarian that was successfully treated with laparoscopic surgery. Although these two forms of hernia are a very rare association, this case report illustrates that the surgical approach should be individualized in each patient's case to ensure a successful surgical outcome. In this case, the decision was made to suture the diaphragmatic crura and reinforce the diaphragm repair with mesh, rather than by fundoplication.
Conflict of interest statement
None.
Figures


References
-
- Loukas M, El-Sedfy A, Tubbs RS, et al. Vincent Alexander Bochdalek (1801–1883) World J Surg. 2008;32:2324–26. - PubMed
-
- Kachlik D, Cech P. Vincenz Alexander Bochdalek (1801–83) J Med Biogr. 2011;19:38–43. - PubMed
-
- Bochdalek VA. Ueber den Peritonealueberzug der Milz und das Ligamentum pleurocolicum. Beitrag zur Anatomie des Bauchfells. Arch Anat Physiol Wiss Med. 1867:565–614. [in German]
-
- Puri P, Wester T. Historical aspects of congenital diaphragmatic hernia. Pediatr Surg Int. 1997;21:95–100. - PubMed
-
- Gedik E, Tuncer MC, Onat S, et al. A review of Morgagni and Bochdalek hernias in adults. Folia Morphol (Warsz) 2011;70:5–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
