

Highly specific reasons for nonadherence to antiretroviral therapy: results from the German adherence study
- PMID: 29184394
- PMCID: PMC5687417
- DOI: 10.2147/PPA.S141762
Highly specific reasons for nonadherence to antiretroviral therapy: results from the German adherence study
Abstract
Background: Reasons for and frequency of nonadherence to antiretroviral therapy (ART) may have changed due to pharmacological improvements. In addition, the importance of known non-pharmacologic reasons for nonadherence is unclear.
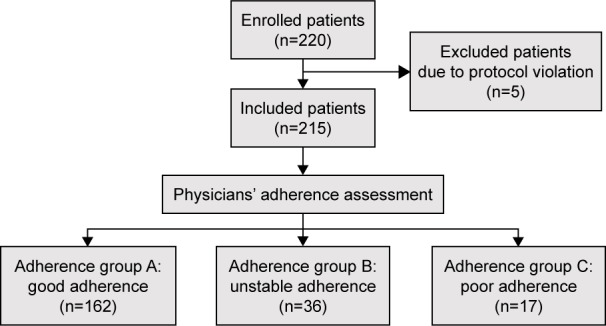
Methods: We performed a cross-sectional, noninterventional, multicenter study to identify current reasons for nonadherence. Patients were categorized by physicians into the following adherence groups: good, unstable, or poor adherence. Co-variables of interest included age, sex, time since HIV diagnosis, ART duration, current ART regimen, HIV transmission route, comorbidity, HIV-1 RNA viral load (VL), and CD4 cell count. Patients self-reported the number of missed doses and provided their specific reasons for nonadherent behavior. Statistical analyses were performed using Fisher's extended exact test, Kruskal-Wallis test, and logistic regression models.
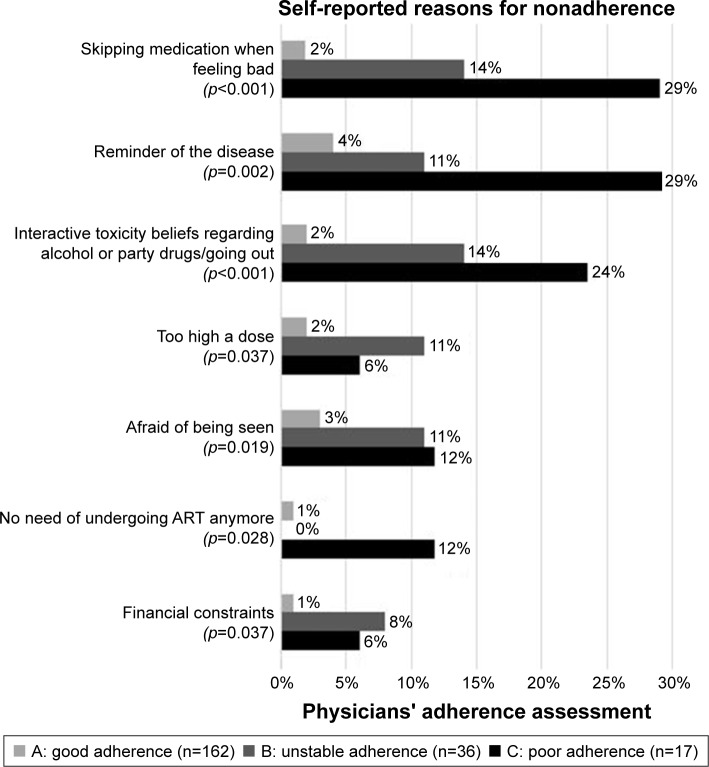
Results: Our study assessed 215 participants with good (n=162), unstable (n=36), and poor adherence (n=17). Compared to patients with good adherence, patients with unstable and poor adherence reported more often to have missed at least one dose during the last week (good 11% vs unstable 47% vs poor 63%, p<0.001). Physicians' adherence assessment was concordant with patients' self-reports of missed doses during the last week (no vs one or more) in 81% cases. Similarly, we found a strong association of physicians' assessment with viral suppression. Logistic regression analysis showed that "reduced adherence" - defined as unstable or poor - was significantly associated with patients <30 years old, intravenous drug use, history of acquired immune deficiency syndrome (AIDS), and psychiatric disorders (p<0.05). Univariate analyses showed that specific reasons, such as questioning the efficacy/dosing of ART, HIV stigma, interactive toxicity beliefs regarding alcohol and/or party drugs, and dissatisfaction with regimen complexity, correlated with unstable or poor adherence (p<0.05).
Conclusion: Identification of factors associated with poor adherence helps in identifying patients with a higher risk for nonadherence. Reasons for nonadherence should be directly addressed in every patient, because they are common and constitute possible adherence intervention points.
Keywords: ART; HIV; adherence; antiretroviral therapy; human immunodeficiency virus; nonadherence; patients’ beliefs.
Conflict of interest statement
Disclosure CW received travel grants from AbbVie, Bristol-Meyers Squibb, Gilead Science, and Jansen. AZ received travel grants from AbbVie, Bristol-Meyers Squibb, Gilead Sciences, and MSD. IK received travel grants from ViiV, Abbvie, MDS, Gilead, and Bristol-Meyers Squibb. The other authors report no conflicts of interest in this work.
Figures
References
-
- Ledergerber B, Cavassini M, Battegay M, et al. Swiss HIV Cohort Study Trends over time of virological and immunological characteristics in the Swiss HIV cohort study. HIV Med. 2011;12(5):279–288. - PubMed
-
- Gulick RM. Adherence to antiretroviral therapy: how much is enough? Clin Infect Dis. 2006;43(7):942–944. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
