

How Should Imaging Direct/Orient Management of Rectal Cancer?
- PMID: 29184465
- PMCID: PMC5703668
- DOI: 10.1055/s-0037-1606107
How Should Imaging Direct/Orient Management of Rectal Cancer?
Abstract
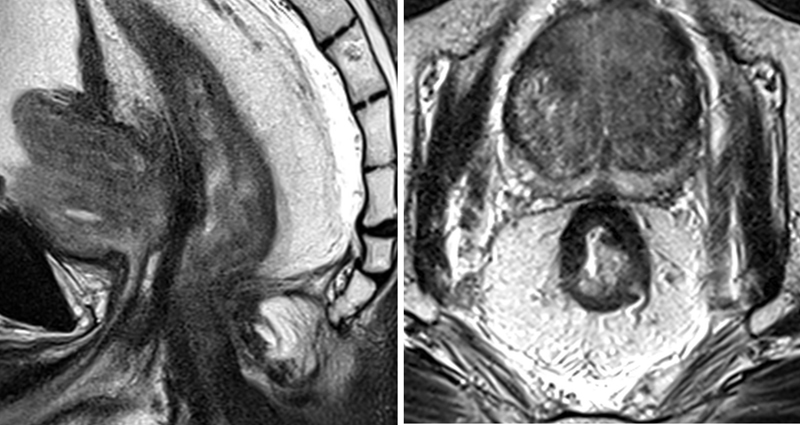
Modern rectal cancer management is dependent on preoperative staging, and radiological assessment is a crucial part of this process. Imaging must provide sufficient information to guide preoperative decision-making that is reliable and reproducible. Different methods have been used for local staging; however, magnetic resonance imaging (MRI) has shown to be the most reliable tool for this purpose. MRI offers prognostic information about the patients and guides the decision between neoadjuvant treatment and total mesorectal excision alone. Also, not only the initial staging but also restaging by MRI can provide significant information regarding tumor response that is essential when considering alternative approaches.
Keywords: local staging; magnetic resonance imaging; rectal cancer.
Figures
References
-
- Battersby N J, Moran B, Yu S, Tekkis P, Brown G. MR imaging for rectal cancer: the role in staging the primary and response to neoadjuvant therapy. Expert Rev Gastroenterol Hepatol. 2014;8(06):703–719. - PubMed
-
- Patel U B, Taylor F, Blomqvist L et al. Magnetic resonance imaging-detected tumor response for locally advanced rectal cancer predicts survival outcomes: MERCURY experience. J Clin Oncol. 2011;29(28):3753–3760. - PubMed
-
- Taylor F G, Swift R I, Blomqvist L, Brown G. A systematic approach to the interpretation of preoperative staging MRI for rectal cancer. AJR Am J Roentgenol. 2008;191(06):1827–1835. - PubMed
-
- Glynne-Jones R, Harrison M, Hughes R. Challenges in the neoadjuvant treatment of rectal cancer: balancing the risk of recurrence and quality of life. Cancer Radiother. 2013;17(07):675–685. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
