

The role of PET/CT imaging in penile cancer
- PMID: 29184780
- PMCID: PMC5673802
- DOI: 10.21037/tau.2017.04.36
The role of PET/CT imaging in penile cancer
Abstract
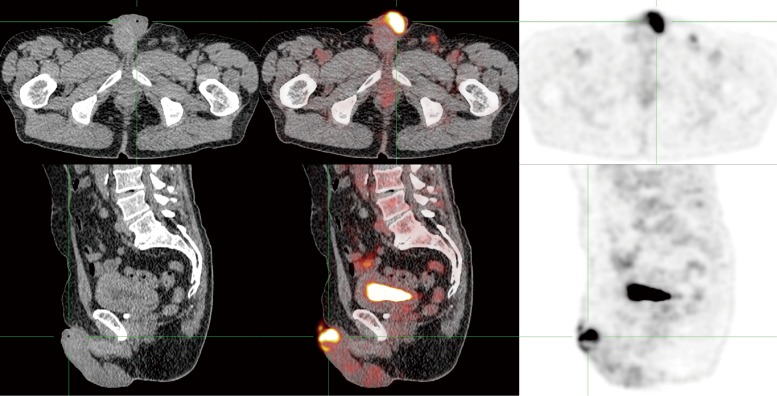
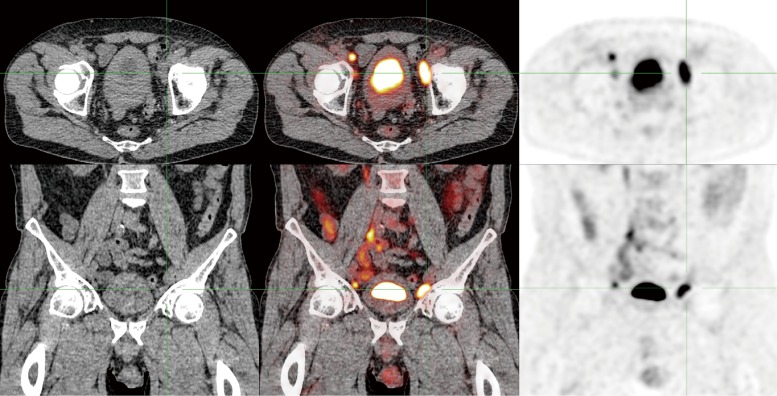
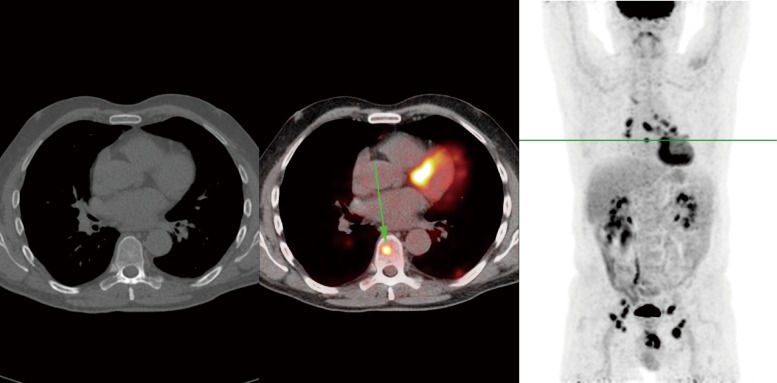
Positron emission tomography (PET) imaging with 18F-fluorodeoxyglucose (FDG) combined with computed tomography (CT) provides functional imaging combined with anatomic information, improving diagnostic accuracy and confidence. Although virtually all primary penile tumors are FDG-avid, PET/CT is not recommended for primary tumor staging as it has limited spatial resolution and is hampered by urinary FDG excretion. The accuracy of PET/CT for lymph node staging seems to improve with the pretest likelihood of metastatic nodes. In groins with normal physical examination, sensitivity is only 57%. In groins with palpably enlarged lymph nodes, sensitivity of PET/CT reaches 96%. For pelvic lymph nodes and distant metastases, PET/CT is more accurate if inguinal metastases are present. However, these results are based on a very limited number of studies. Overall, the role of PET/CT imaging in penile cancer remains ambiguous, especially in inguinal lymph nodes. During staging and follow-up, it may be particularly useful in detecting pelvic lymph node metastases and occult distant metastases prior to systemic chemotherapy and/or extensive surgery, improving selection of patients that are most likely to benefit from such therapies.
Keywords: 18F-fluorodeoxyglucose (FDG); PET/CT; Penile cancer; fluorodeoxyglucose; imaging.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources