

Functional status mediates the association between peripheral neuropathy and health-related quality of life in individuals with diabetes
- PMID: 29185052
- PMCID: PMC5816102
- DOI: 10.1007/s00592-017-1077-8
Functional status mediates the association between peripheral neuropathy and health-related quality of life in individuals with diabetes
Abstract
Aims: To examine differences in health-related quality of life (HRQoL) between patients with and without diabetic peripheral neuropathy (DPN), and whether these differences can be explained by functional deficits.
Methods: This was a cross-sectional study of 160 patients with type 2 diabetes mellitus, 80 with DPN and 80 without. Assessments included HRQoL (health utility score derived from EQ-5D-5L), functional status measurements [muscle strength, timed up and go (TUG), five times sit-to-stand (FTSTS), functional reach, body sway velocity] and self-reported balance confidence [Activities-specific Balance Confidence (ABC) scale].
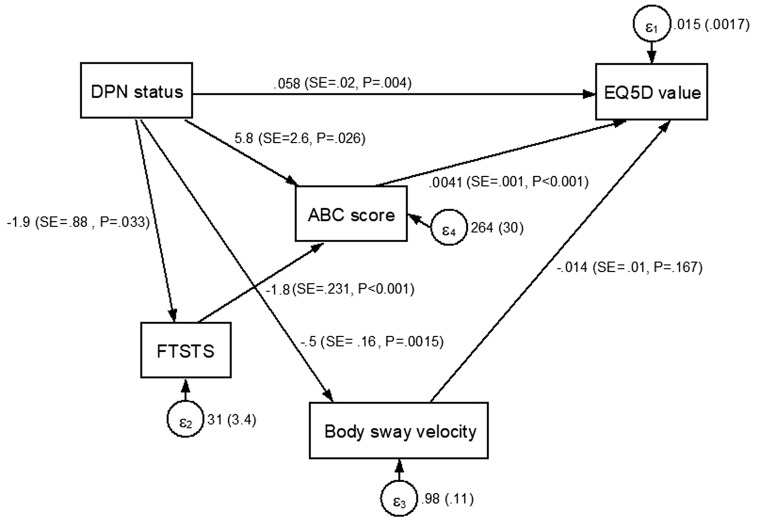
Results: Mean utility scores were 0.67 ± 0.14 and 0.77 ± 0.16 in patients with and without DPN, respectively (p < 0.001). Patients with DPN had lower great toe extensor strength (6.4 ± 1.8 vs 7.6 ± 2.8 lbs, p = 0.001), greater body sway velocity (2.40 ± 1.31 vs 1.90 ± 0.52 mm/s, p = 0.002), slower TUG (12.1 ± 4.6 vs 10.1 ± 2.3 s, p < 0.001) and FTSTS (15.8 ± 5.8 vs 13.9 ± 5.4 s, p = 0.03) scores, and lower ABC score (73.4 ± 21.3 vs 82.6 ± 16.9, p = 0.003), compared to those without DPN. On stepwise multiple regression, DPN status, FTSTS, body sway velocity, BMI, diabetes duration, pain, and gender explained 38% of HRQoL variance. Addition of ABC score into the model explained 45% of variance. Results from structural equation modelling showed that DPN had direct effects on HRQoL and indirect effects through FTSTS, body sway velocity, and ABC score, with χ 2 = 8.075 (p = 0.044), root mean square error of approximation = 0.103 (lower bound 0.015, upper bound 0.191), Comparative Fit Index = 0.966, Tucker-Lewis Index = 0.887, and Standardized Root Mean Square Residual = 0.053.
Conclusions: Patients with DPN have worse HRQoL compared to patients without DPN, partly mediated by functional status parameters. Effective interventions targeting functional status may be beneficial in improving HRQoL in these patients.
Keywords: Diabetic polyneuropathy; Functional status; Health-related quality of life; Muscle strength; Postural balance; Range of motion; Type 2 diabetes mellitus.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Ethical approval was obtained from the National Healthcare Group Domain Specific Review Board and SingHealth Centralised Institutional Review Board.
Informed consent
Written informed consent was obtained from all participants prior to study initiation.
Figures

References
-
- Grandy S, Fox KM. EQ-5D visual analog scale and utility index values in individuals with diabetes and at risk for diabetes: findings from the study to help improve early evaluation and management of risk factors leading to diabetes (SHIELD) Health Q Life Outcomes. 2008;6(1):1. doi: 10.1186/1477-7525-6-1. - DOI - PMC - PubMed
-
- Dyck PJ, Kratz K, Karnes J, Litchy WJ, Klein R, Pach J, Wilson D, O’Brien P, Melton L. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort The Rochester Diabetic Neuropathy Study. Neurology. 1993;43(4):817-817. doi: 10.1212/WNL.43.4.817. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
