

Incremental Prognostic Value of Conventional Echocardiography in Patients with Acutely Decompensated Heart Failure
- PMID: 29185616
- PMCID: PMC5783437
- DOI: 10.5935/abc.20170173
Incremental Prognostic Value of Conventional Echocardiography in Patients with Acutely Decompensated Heart Failure
Abstract
Background: Acutely decompensated heart failure (ADHF) presents high morbidity and mortality in spite of therapeutic advance. Identifying factors of worst prognosis is important to improve assistance during the hospital phase and follow-up after discharge. The use of echocardiography for diagnosis and therapeutic guidance has been of great utility in clinical practice. However, it is not clear if it could also be useful for risk determination and classification in patients with ADHF and if it is capable of adding prognostic value to a clinical score (OPTIMIZE-HF).
Objective: To identify the echocardiographic variables with independent prognostic value and to test their incremental value to a clinical score.
Methods: Prospective cohort of patients consecutively admitted between January 2013 and January 2015, with diagnosis of acutely decompensated heart failure, followed up to 60 days after discharge. Inclusion criteria were raised plasma level of NT-proBNP (> 450 pg/ml for patients under 50 years of age or NT-proBNP > 900 pg/ml for patients over 50 years of age) and at least one of the signs and symptoms: dyspnea at rest, low cardiac output or signs of right-sided HF. The primary outcome was the composite of death and readmission for decompensated heart failure within 60 days.
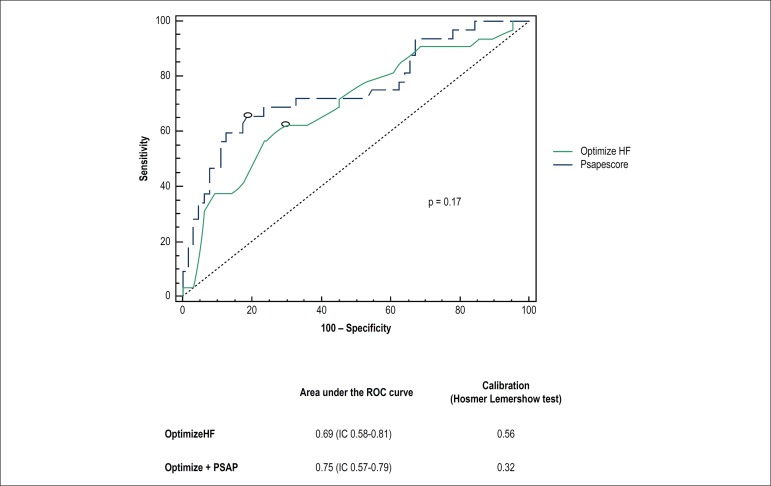
Results: Study participants included 110 individuals with average age of 68 ± 16 years, 55% male. The most frequent causes of decompensation (51%) were transgression of the diet and irregular use of medication. Reduced ejection fraction (<40%) was present in 47% of cases, and the NT-proBNP median was 3947 (IIQ = 2370 to 7000). In multivariate analysis, out of the 16 echocardiographic variables studied, only pulmonary artery systolic pressure remained as an independent predictor, but it did not significantly increment the C-statistic of the OPTMIZE-HF score.
Conclusion: The addition of echocardiographic variables to the OPTIMIZE-HF score, with the exception of left ventricular ejection fraction, did not improve its prognostic accuracy concerning cardiovascular events (death or readmission) within 60 days.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, et al. ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):603–669. doi: 10.1093/eurjhf/hfs105. - DOI - PubMed
-
- Fonarow GC. The treatment target in acute decompensated heart failure. Rev Cardiovasc Med. 2001;2(Suppl 2):s7–s12. - PubMed
-
- American Heart Association . Heart and stroke statistical update. Dallas(USA): AHA; 2002. Available from: http://www.heart.org/HEARTORG/General/Heart-and-Stroke-Association-Stati....
-
- Schocken DD, Benjamin EJ, Fonarow GC, Krumholz HM, Levy D, Mensah GA, et al. Prevention of heart failure: a scientific statement from the American Heart Association Councils on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular Nursing, and High Blood Pressure Research; Quality of Care and Outcomes Research Interdisciplinary Working Group; and Functional Genomics and Translational Biology Interdisciplinary Working Group. Circulation. 2008;117(19):2544–2565. doi: 10.1161/CIRCULATIONAHA.107.188965. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
