

Case Reports
Transplantation of multiple abdominal viscera
Affiliations
- PMID: 2918640
- PMCID: PMC3005343
Item in Clipboard
Case Reports
Transplantation of multiple abdominal viscera
JAMA.
.
Abstract
Two children with the short-gut syndrome and secondary liver failure were treated with evisceration and transplantation en bloc of the stomach, small intestine, colon, pancreas, and liver. The first patient died perioperatively, but the second lived for more than 6 months before dying of an Epstein-Barr virus-associated lymphoproliferative disorder that caused biliary obstruction and lethal sepsis. There was never evidence of graft rejection or of graft-vs-host disease in the long-surviving child. The constituent organs of the homograft functioned and maintained their morphological integrity throughout the 193 days of survival.
Figures
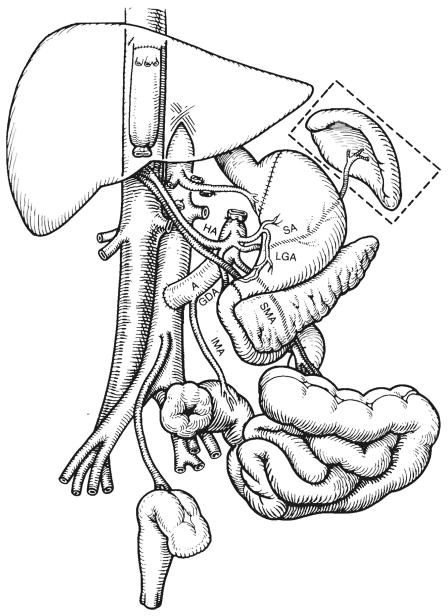
The recipient operation of multivisceral transplantation. Note that the venous outflow of the graft was into a cloaca of the left and middle hepatic veins, leaving the recipient inferior vena cava intact. A indicates donor aorta; HA, hepatic artery; SA, splenic artery; LGA, left gastric artery; SMA, superior mesenteric artery; IMA, inferior mesenteric artery; and GDA, gastro-duodenal artery.
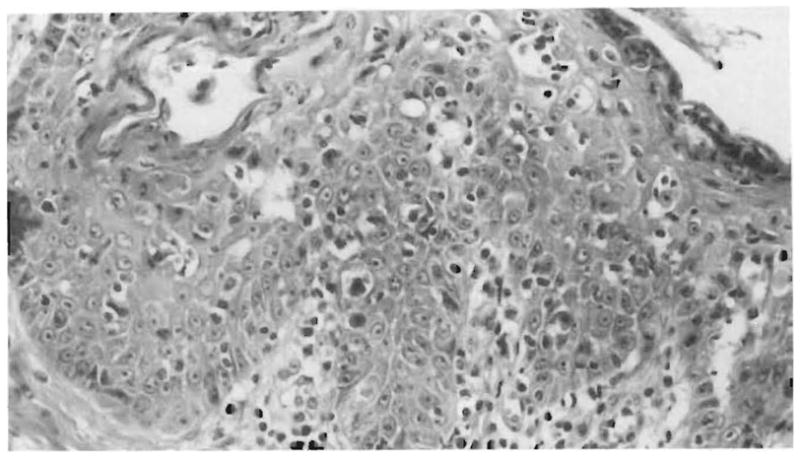
Skin biopsy from a pig 14 days after multivisceral transplantation. Note the lymphocytic infiltrate at the dermal-epidermal junction and lymphocytes in proximity to necrotic epithelial cells (satellitosis) (hematoxylineosin, × 350).
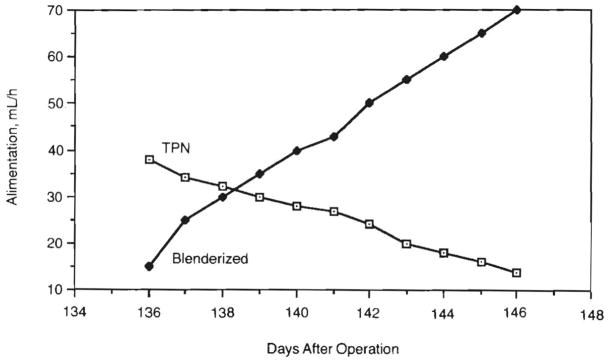
Enteral and parenteral alimentation. As a blenderized diet was increased, we were able to gradually reduce total parental hyperalimentation (TPN) to a very low level.
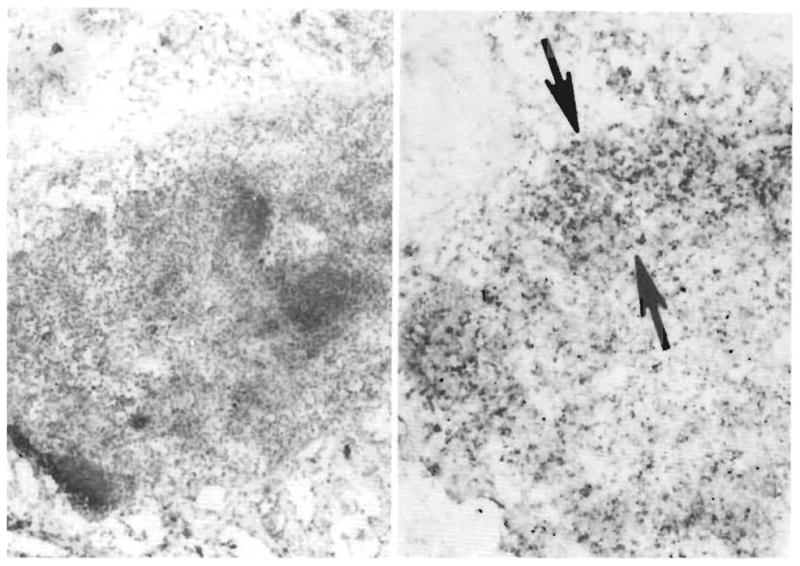
Demonstration of OKT3. Left, A small mesenteric donor lymph node is embedded in fat (frozen section, pinocyanol, × 110), Right, Some cells in the nodal sinuses, cortex, and paracortex (arrows) stain darkly for the presence of murine IgG (alkaline phosphatase/antialkaline phosphatase, × 110).
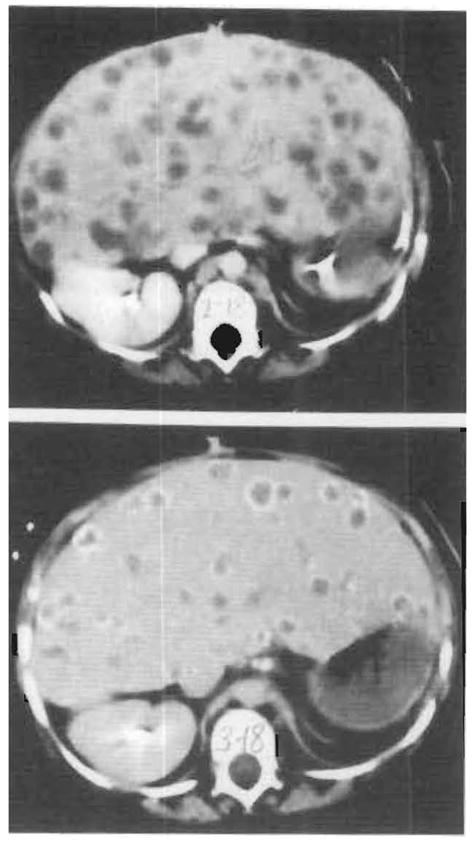
Computed tomographic scans of initial lymphoproliferative disease process. Top, One hundred nine days after transplantation. Multiple lucencies within the liver parenchyma are seen. Histological examination of the cells obtained on liver biopsy revealed a polyclonal lymphoproliferative disorder (see Fig 6, right). Bottom, One hundred thirty-seven days after transplantation. Calcific rims surround many of the parenchymal lucencies. Histological examination revealed necrotic lymphoproliferative cells (see Fig 6, center).
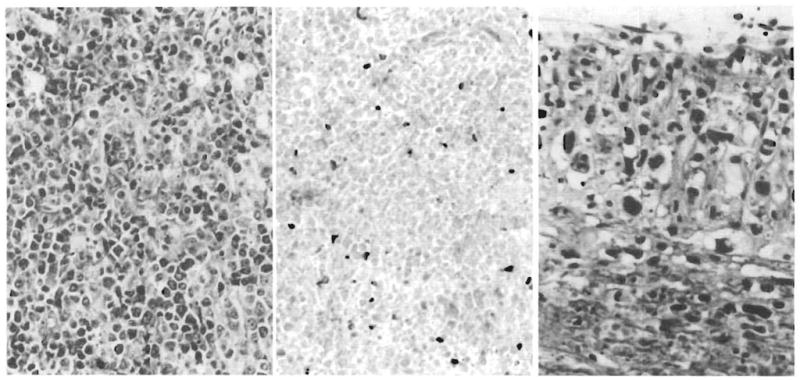
Allograft liver, lymphoproliferative disease. Left, Allograft liver biopsy specimen at 3 months. A diffuse plasmacytoid lymphoid proliferation destroys hepatic tissue (Giemsa, ×220). Center, Allograft liver biopsy specimen at 3¾ months. Necrotic lymphoproliferative disease is represented by ghost cells that have lost both nuclear and cytoplasmic staining detail. Occasional nucleated inflammatory cells persist (hematoxylin-eosin, × 240). Right, Hepatic hilar vasculitis present at autopsy. Branches of the hepatic artery, the hilar fibrous tissue, head of pancreas, and adjacent colon are permeated by a very polymorphous, anaplastic-looking infiltrate quite different from the earlier lymphoproliferative disorder (hematoxylin-eosin, × 440).
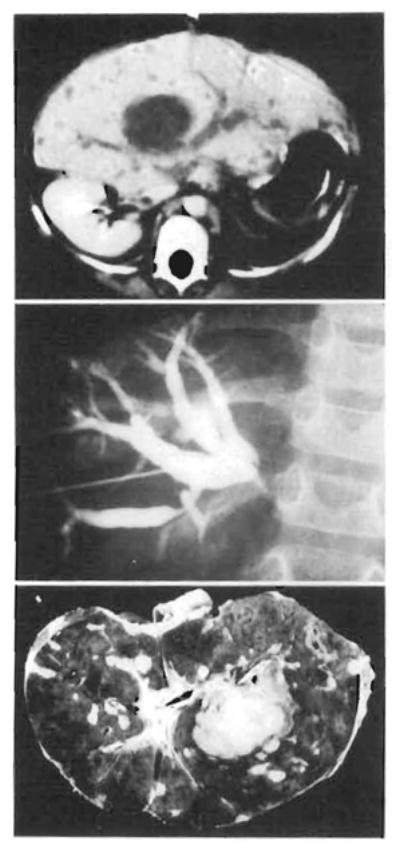
Computed tomographic scan and cholangiogram of terminal lymphoproliferative disease process and the hemisected liver at autopsy. Top, Computed tomographic scan at 165 days. The hepatic ducts are obstructed by a large hilar mass discovered on histological examination to be morphologically different than the previous lymphoproliferative disease process (see Fig 6, right). This was confirmed by transhepatic cholangiogram (center). Note the resolving lymphoproliferative disease in the periphery of the liver on the computed tomographic scan, Bottom, Transected liver at autopsy confirms previously mentioned findings and reveals widespread parenchymal necrosis with hemorrhage. Note catheters within the hepatic ducts.
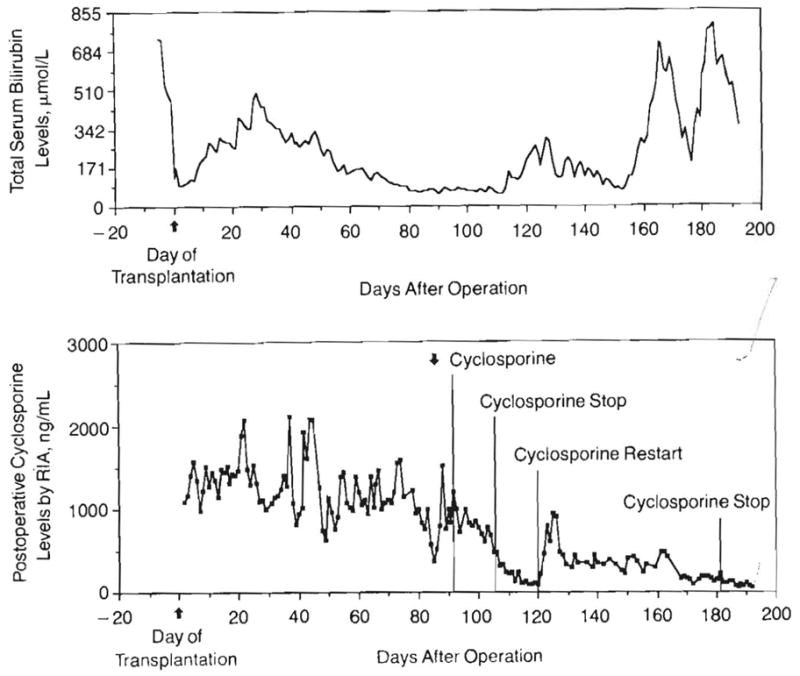
Parallel graphs of serum total bilirubin levels and cyclosporine (radioimmunoassay [RIA]) levels. Four major findings: (1) Rapid fall in total bilirubin level immediately after transplantation, (2) Progressive rise in bilirubin level from days 7 to 30. OKT3 administered for one week beginning day 23 with a decline to normal after treatment. (3) No rise in bilirubin level is seen during the early lymphproliferative disease (day 91). Cyclosporine was subsequently stopped but restarted due to fear of potential rejection or graft-vs-host disease. (4) Late, rapid rise of bilirubin level caused by the obstructing, fatal lymphoproliferative disease that was only transiently relieved by biliary catheter drainage.
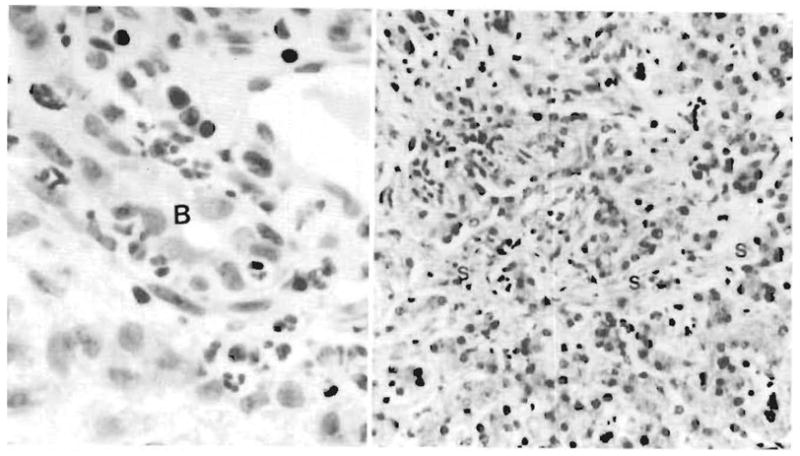
Allograft liver. Left, Biopsy specimen obtained on day 11 after transplantation reveals a cholangitis and pericholangitis. Neutrophils are present in and around a bile duct (B). Right, Allograft liver biopsy specimen obtained at 6 months. The liver has canalicular cholestasis, bile ductular proliferation, and a generalized fine sinusoidal fibrosis (S) believed to be most consistent with prolonged hyperalimentation effect (hematoxylineosin, ×200).

Barium meal–day 109. Note the feathery normal appearance of the small intestine mucosa.
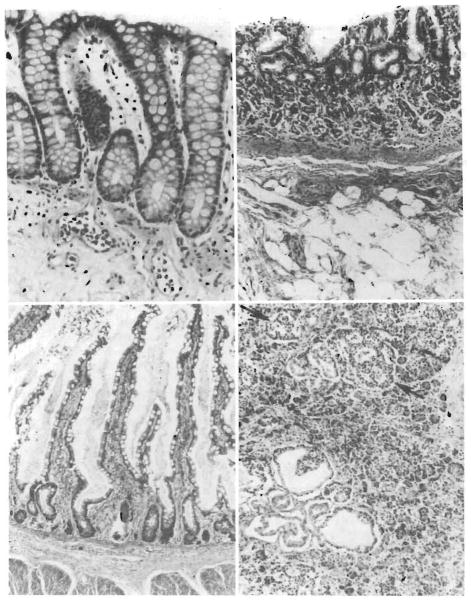
Gastrointestinal tract. Top left, Colonic biopsy specimen from the donor colon proximal to the colostomy, taken 1 week before death (6 months after transplant). The glands extend to the muscularis mucosae, a normal finding, and there is neither cellular infiltration nor epithelial damage. Lymphoid tissue is sparse (hematoxylin-eosin, ×280). Top right, Donor stomach at autopsy. The mucosa has mild atrophy and some fibrosis of the lamina propria (hematoxylin-eosin, ×180). Bottom left, Donor ileum at autopsy. In places, the villous architecture reveals hyperplasia rather than atrophy. The surface epithelium is intact, the lamina propria somewhat fibrotic, but there is no cellular infiltrate (hematoxylin-eosin, ×150) Bottom right, Donor pancreas at autopsy. There are foci of cystic ductular proliferation in the head of the pancreas. For the most part, islets are abundant (arrows) and there is little atrophy, interstital fibrosis or cellular infiltrate (hematoxylin-eosin, ×180).
References
-
- Nalesnik MA, Makowka L, Starzl TE. The diagnosis and treatment of post-transplant lymphoproliferative disorders. Curr Probl Surg. 1988;25:365–472. - PubMed
-
- Williams JW, Sankary HN, Foster PF, Lowe J, Goldman GM. Splanchnic transplantation: an approach to the infant dependent on parenteral nutrition who develops irreversible liver disease. JAMA. 1989;261:1458–1462. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
