

Protection of the Human Gut Microbiome From Antibiotics
- PMID: 29186529
- PMCID: PMC5853327
- DOI: 10.1093/infdis/jix604
Protection of the Human Gut Microbiome From Antibiotics
Abstract
Background: Antibiotics are life-saving drugs but severely affect the gut microbiome with short-term consequences including diarrhea and selection of antibiotic-resistant bacteria. Long-term links to allergy and obesity are also suggested. We devised a product, DAV132, and previously showed its ability to deliver a powerful adsorbent, activated charcoal, in the late ileum of human volunteers.
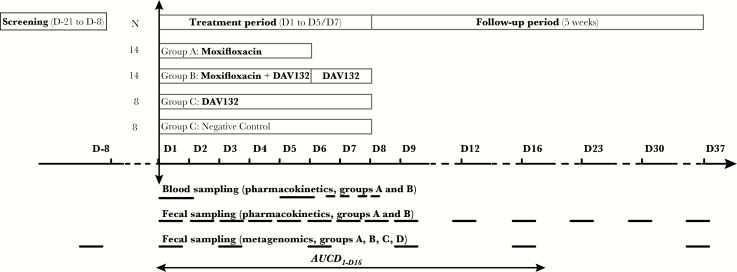
Methods: We performed a randomized controlled trial in 28 human volunteers treated with a 5-day clinical regimen of the fluoroquinolone antibiotic moxifloxacin in 2 parallel groups, with or without DAV132 coadministration. Two control goups of 8 volunteers each receiving DAV132 alone, or a nonactive substitute, were added.
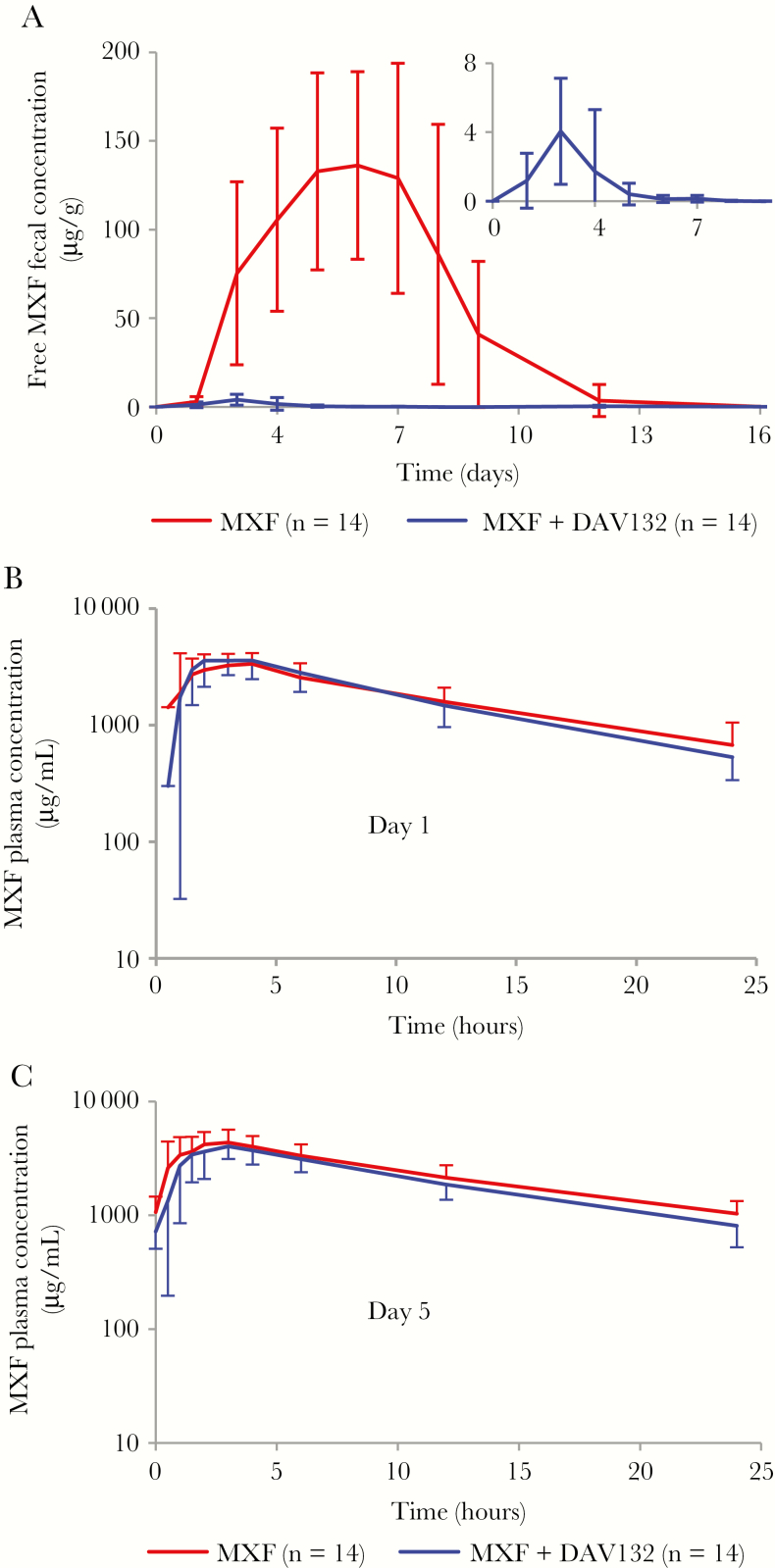
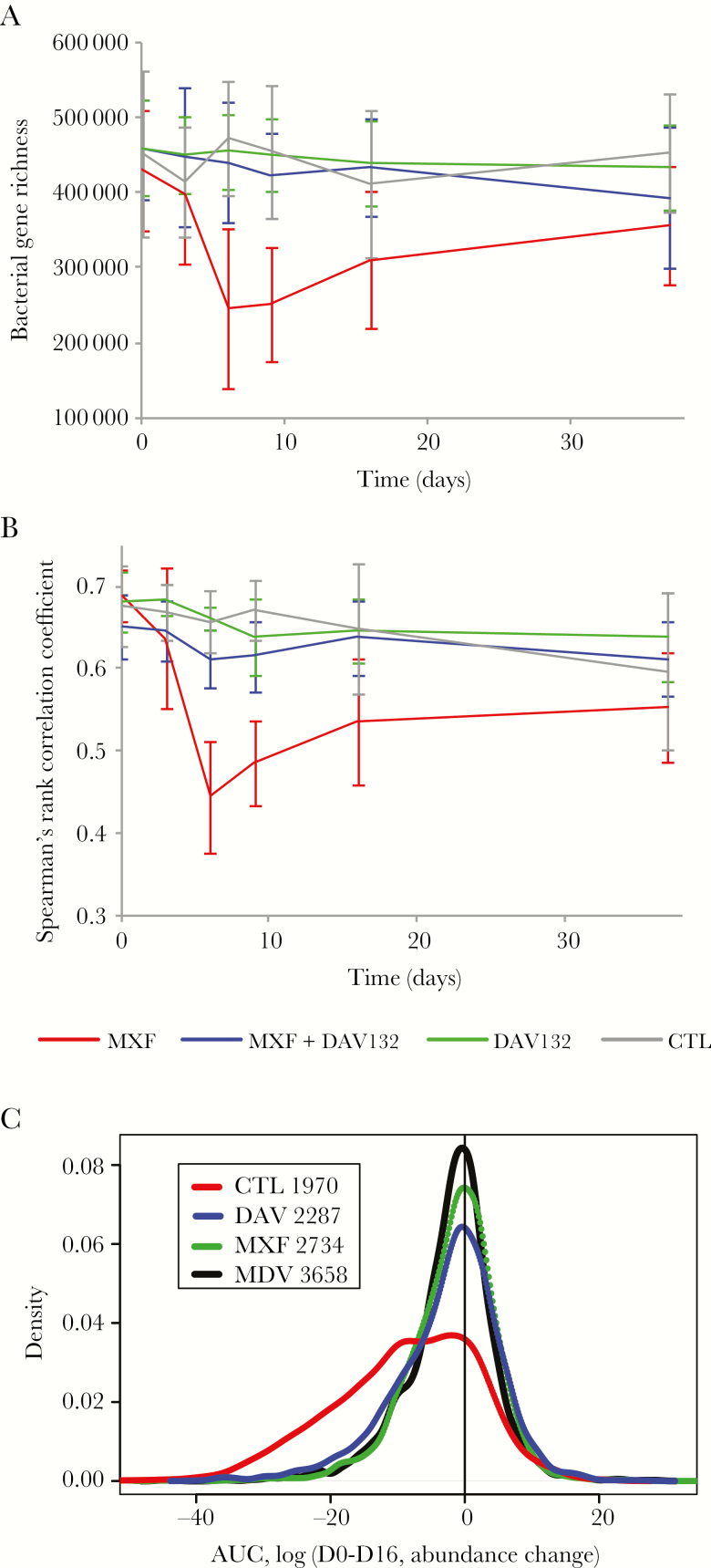
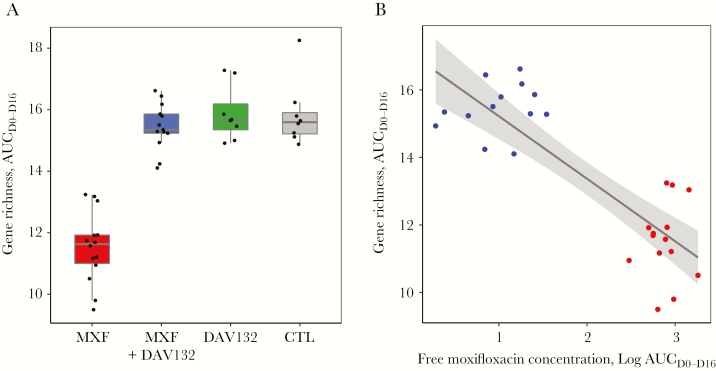
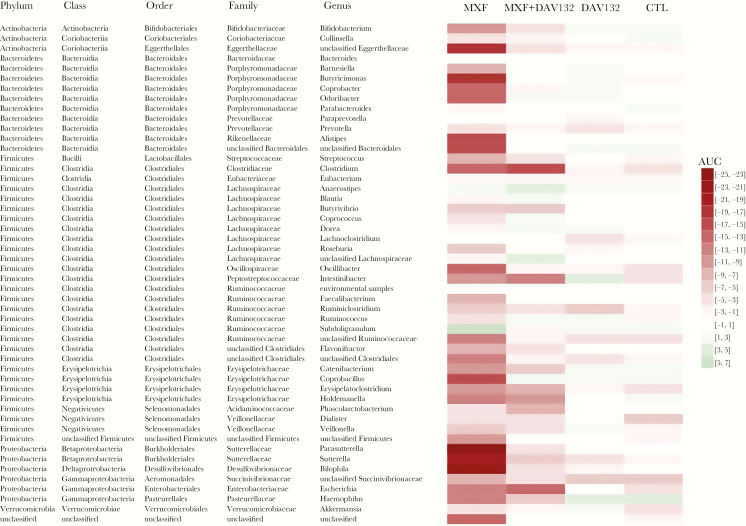
Results: The coadministration of DAV132 decreased free moxifloxacin fecal concentrations by 99%, while plasmatic levels were unaffected. Shotgun quantitative metagenomics showed that the richness and composition of the intestinal microbiota were largely preserved in subjects co-treated with DAV132 in addition to moxifloxacin. No adverse effect was observed. In addition, DAV132 efficiently adsorbed a wide range of clinically relevant antibiotics ex vivo.
Conclusions: DAV132 was highly effective to protect the gut microbiome of moxifloxacin-treated healthy volunteers and may constitute a clinical breakthrough by preventing adverse health consequences of a wide range of antibiotic treatments.
Clinical trials registration: NCT02176005.
Keywords: Clostridium difficile; antibiotics; fluoroquinolones; microbiome.
© The Author(s) 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Jernberg C, Löfmark S, Edlund C, Jansson JK. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiology 2010; 156:3216–23. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
