

Massive pelvic recurrence of uterine leiomyomatosis with intracaval-intracardiac extension: video case report and literature review
- PMID: 29187188
- PMCID: PMC5707788
- DOI: 10.1186/s12893-017-0306-y
Massive pelvic recurrence of uterine leiomyomatosis with intracaval-intracardiac extension: video case report and literature review
Abstract
Background: Uterine leiomyomas represent the gynecological neoplasm with the highest prevalence worldwide. This apparently benign pathological entity may permeate into the venous system causing the so-called intravenous leiomyomatosis of the uterus (IVL). IVL may seldom extend to large caliber veins and reach the right cardiac chambers or pulmonary arteries and cause signs of right sided congestive heart failure and sudden death. Due to its low incidence, however, IVL with intracardiac extension is often misdiagnosed resulting in deferred treatment. No consensus has been obtained regarding the standard surgical approach to be used for this rare condition. We describe the case of a massive pelvic recurrence of uterine leiomyomatosis with intracardiac extension and provide a review of the literature, analyzing management and surgical outcomes.
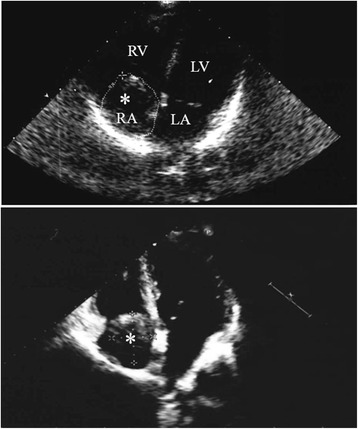
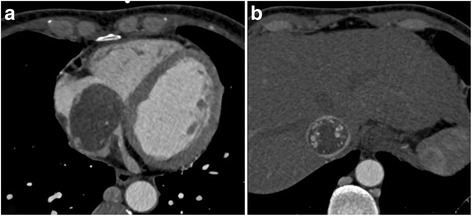
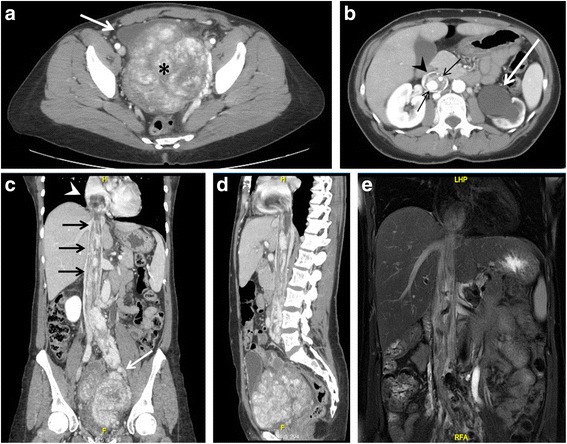
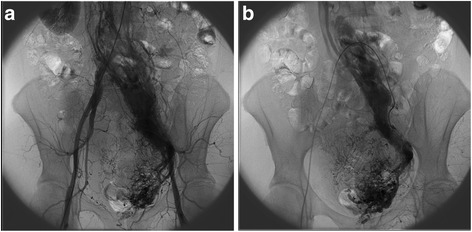
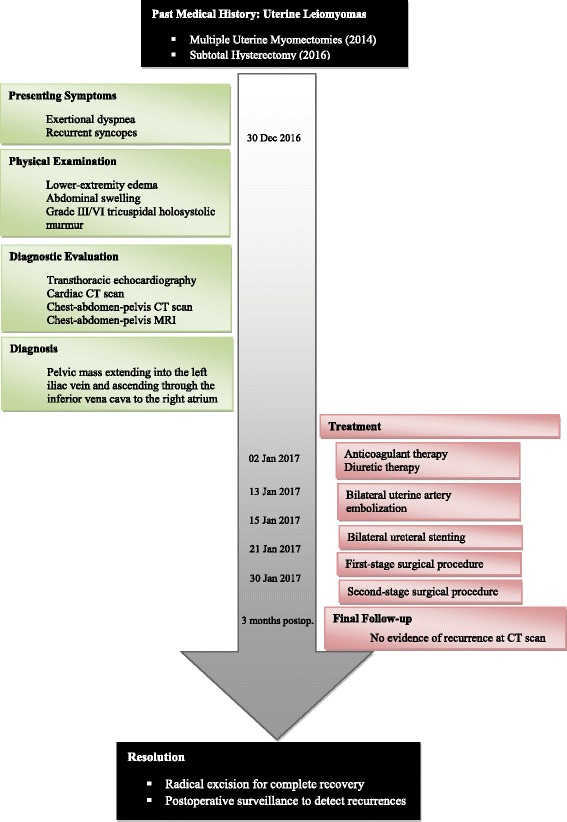
Case presentation: We present the case of a 46-year-old premenopausal woman presenting with lower-extremity edema, recurrent syncopes and a history of subtotal hysterectomy for multiple uterine fibroids. She was diagnosed with pelvic recurrence of uterine leiomyomatosis and IVL with cardiac involvement. A two-stage surgical excision of the intracardiac-intracaval mass and pelvic leiomyomatosis was performed. The patient had an uneventful recovery and no evidence of recurrence was observed on follow-up.
Conclusions: By virtue of the rarity of the present pathology, awareness is widely scarce and diagnosis is often delayed. Early recognition is difficult due to initial aspecific and subtle clinical manifestations. Nevertheless, suspicion should be held high in premenopausal women with known history of uterine leiomyomata, presenting with cardiovascular symptoms and evidence of a free-floating mass within the right cardiac chambers. In-depth imaging is crucial for defining its anatomical origin and relations. Prompt surgical treatment with radical excision of pelvic and intravenous leiomyomatosis guarantees favorable outcomes and excellent prognosis with low rates of recurrence, whereas delayed diagnosis and treatment exposes to increased risk of congestive heart failure and sudden death.
Keywords: Cardiopulmonary bypass; Hysterectomy; Intracardiac leiomyomatosis; Intravenous leiomyomatosis; Uterine leiomyoma.
Conflict of interest statement
Ethics approval and consent to participate
The study was reviewed and approved by the institutional human ethics committee in accordance with National guidelines and the provisions of the Helsinki Declaration, as revised in 2000. The patient provided written informed consent to participate in the study, and additional written informed consent was obtained before surgery.
Consent for publication
Written informed consent to this case report was obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Birch-Hirschfeld, F. V.: Lehrbuch der Pathologischen Anatomie. 5th Ed. Leipzig. F. C. W. Vogel, 1896.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
