

Phenotyping of Sleep-Disordered Breathing in Patients With Chronic Heart Failure With Reduced Ejection Fraction-the SchlaHF Registry
- PMID: 29187390
- PMCID: PMC5778994
- DOI: 10.1161/JAHA.116.005899
Phenotyping of Sleep-Disordered Breathing in Patients With Chronic Heart Failure With Reduced Ejection Fraction-the SchlaHF Registry
Abstract
Background: Different sleep-disordered breathing (SDB) phenotypes, including coexisting obstructive and central sleep apnea (OSA-CSA), have not yet been characterized in a large sample of patients with heart failure and reduced ejection fraction (HFrEF) receiving guideline-based therapies. Therefore, the aim of the present study was to determine the proportion of OSA, CSA, and OSA-CSA, as well as periodic breathing, in HFrEF patients with SDB.
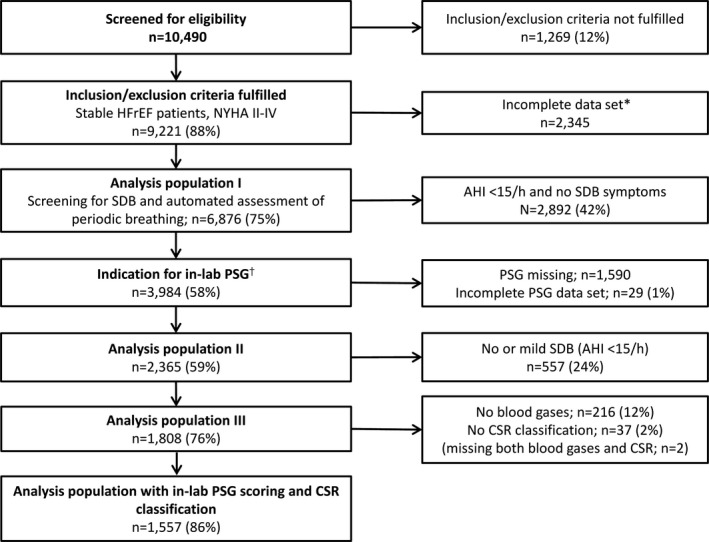
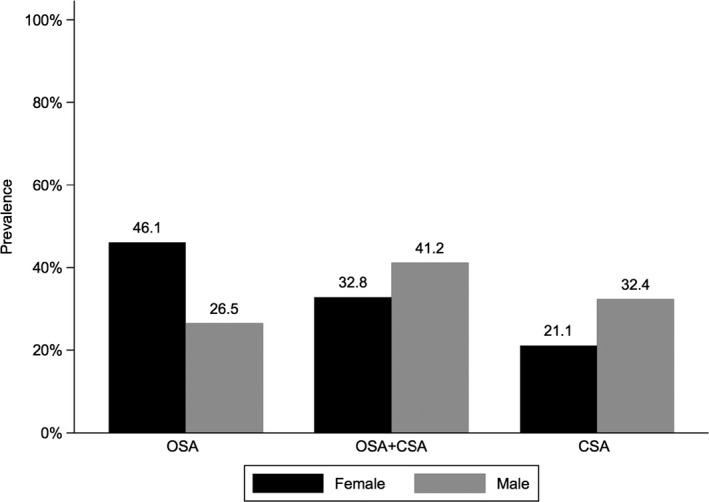
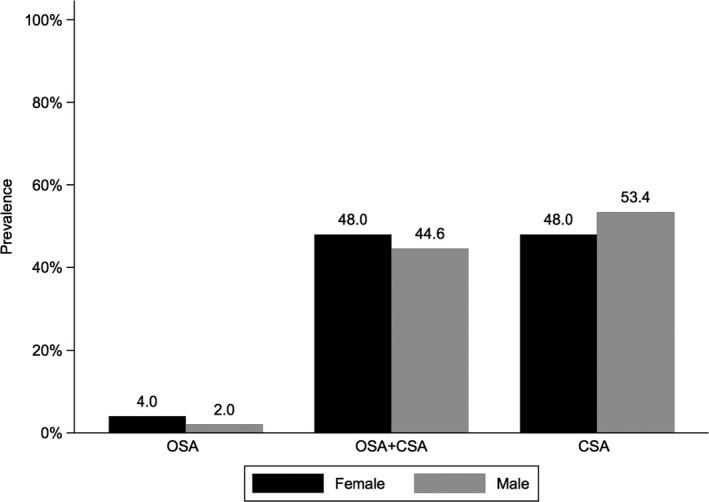
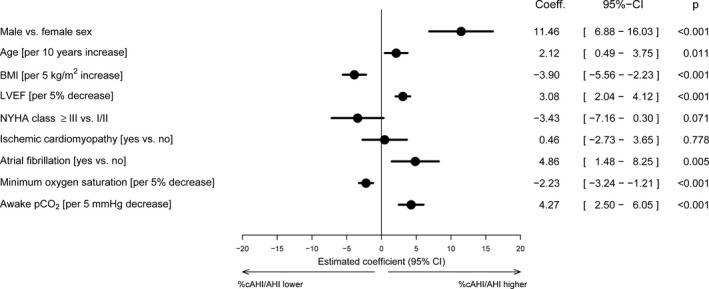
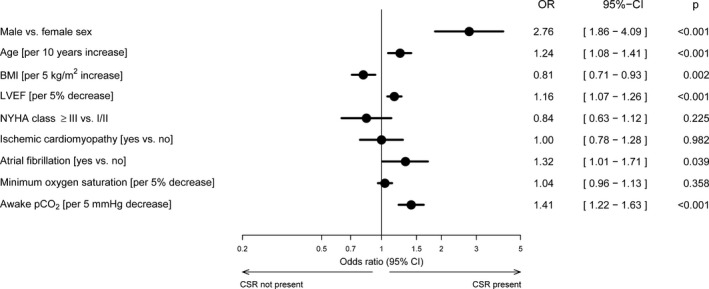
Methods and results: The German SchlaHF registry enrolled patients with HFrEF receiving guideline-based therapies, who underwent portable SDB monitoring. Polysomnography (n=2365) was performed in patients with suspected SDB. Type of SDB (OSA, CSA, or OSA-CSA), the occurrence of periodic breathing (proportion of Cheyne-Stokes respiration ≥20%), and blood gases were determined in 1557 HFrEF patients with confirmed SDB. OSA, OSA-CSA, and CSA were found in 29%, 40%, and 31% of patients, respectively; 41% showed periodic breathing. Characteristics differed significantly among SDB groups and in those with versus without periodic breathing. There was a relationship between greater proportions of CSA and the presence of periodic breathing. Risk factors for having CSA rather than OSA were male sex, older age, presence of atrial fibrillation, lower ejection fraction, and lower awake carbon dioxide pressure (pco2). Periodic breathing was more likely in men, patients with atrial fibrillation, older patients, and as left ventricular ejection fraction and awake pco2 decreased, and less likely as body mass index increased and minimum oxygen saturation decreased.
Conclusions: SchlaHF data show that there is wide interindividual variability in the SDB phenotype of HFrEF patients, suggesting that individualized management is appropriate.
Clinical trial registration: URL: https://www.clinicaltrials.gov/. Unique identifier: NCT01500759.
Keywords: heart failure; phenotypes; sleep apnea; sleep disorders.
© 2017 The Authors and ResMed Germany Inc. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J Am Coll Cardiol. 2004;43:317–327. - PubMed
-
- McCullough PA, Philbin EF, Spertus JA, Kaatz S, Sandberg KR, Weaver WD. Resource utilization among congestive heart failure study. Confirmation of a heart failure epidemic: findings from the Resource Utilization Among Congestive Heart Failure (REACH) study. J Am Coll Cardiol. 2002;39:60–69. - PubMed
-
- Roger VL, Go AS, Lloyd‐Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2012 update: a report from the American Heart association. Circulation. 2012;125:e2–e220. - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
