

Impact of inhalational versus intravenous anaesthesia on early delirium and long-term survival in elderly patients after cancer surgery: study protocol of a multicentre, open-label, and randomised controlled trial
- PMID: 29187413
- PMCID: PMC5719291
- DOI: 10.1136/bmjopen-2017-018607
Impact of inhalational versus intravenous anaesthesia on early delirium and long-term survival in elderly patients after cancer surgery: study protocol of a multicentre, open-label, and randomised controlled trial
Abstract
Introduction: Elderly patients who have solid organ cancer often receive surgery. Some of them may develop delirium after surgery and delirium development is associated with worse outcomes. Furthermore, despite all of the advances in medical care, the long-term survival in cancer patients is far from optimal. Evidences suggest that choice of anaesthetics during surgery, that is, either inhalational or intravenous anaesthetics, may influence outcomes. However, the impact of general anaesthesia type on the occurrence of postoperative delirium is inconclusive. Although retrospective studies suggest that propofol-based intravenous anaesthesia was associated with longer survival after cancer surgery when compared with inhalational anaesthesia, prospective studies as such are still lacking. The purposes of this randomised controlled trial are to test the hypotheses that when compared with sevoflurane-based inhalational anaesthesia, propofol-based intravenous anaesthesia may reduce the incidence of early delirium and prolong long-term survival in elderly patients after major cancer surgery.
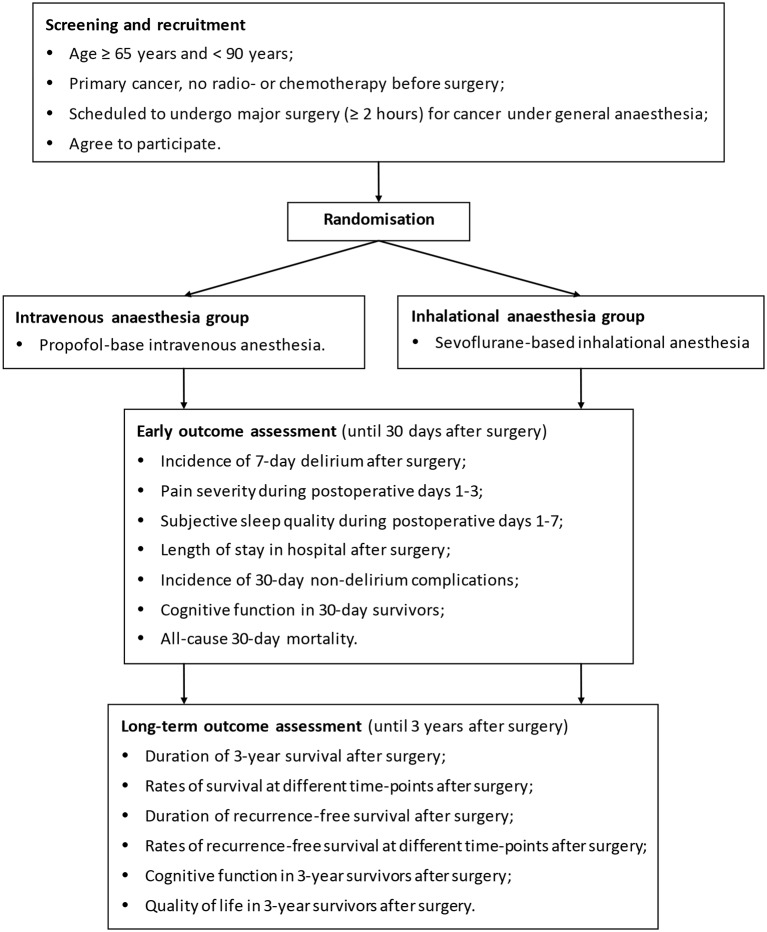
Methods and analysis: This is a multicentre, open-label, randomised controlled trial with two parallel arms. 1200 elderly patients (≥65 years but <90 years) who are scheduled to undergo major cancer surgery (with predicted duration ≥2 hours) are randomised to receive either sevoflurane-based inhalational anaesthesia or propofol-based intravenous anaesthesia. Other anaesthetics and supplemental drugs including sedatives, opioids and muscle relaxants are administered in both arms according to routine practice. The primary early outcome is the incidence of 7-day delirium after surgery and the primary long-term outcome is the duration of 3-year survival after surgery.
Ethics and dissemination: The study protocol has been approved by the Clinical Research Ethics Committees of Peking University First Hospital (2015[869]) and all participating centres. The results of early and long-term outcomes will be analysed and reported separately.
Trial registration number: ChiCTR-IPR-15006209; NCT02662257; NCT02660411.
Keywords: anaesthesia in oncology; cancer; surgery; survival.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: DXW is supported by grants from the Wu Jieping Medical Foundation(320.6750.15175), China and the Chinese Society of Cardiothoracic and Vascular Anesthesiology, China; he reports lecture fees and travel expenses for lectures from Jiangsu Hengrui Medicine Co Ltd, China, Yichang Humanwell Pharmaceutical Co Ltd, China, and Jiangsu Nhwa Pharmaceutical Co Ltd, China. DM is supported by grants from the British Oxygen Chair, and British Journal of Anaesthesia Fellowship, London, UK.
Similar articles
-
A multicentre, randomised, open-label, controlled trial evaluating equivalence of inhalational and intravenous anaesthesia during elective craniotomy.Eur J Anaesthesiol. 2012 Aug;29(8):371-9. doi: 10.1097/EJA.0b013e32835422db. Eur J Anaesthesiol. 2012. PMID: 22569025 Clinical Trial.
-
Early postoperative cognitive dysfunction and postoperative delirium after anaesthesia with various hypnotics: study protocol for a randomised controlled trial--the PINOCCHIO trial.Trials. 2011 Jul 6;12:170. doi: 10.1186/1745-6215-12-170. Trials. 2011. PMID: 21733178 Free PMC article. Clinical Trial.
-
Effect of desflurane, sevoflurane or propofol on the incidence of postoperative delirium in older adults undergoing moderate- to high-risk major non-cardiac surgery: study protocol for a prospective, randomised, observer-blinded, clinical trial (RAPID-II trial).BMJ Open. 2024 Nov 27;14(11):e092611. doi: 10.1136/bmjopen-2024-092611. BMJ Open. 2024. PMID: 39609026 Free PMC article.
-
Propofol vs. inhalational agents to maintain general anaesthesia in ambulatory and in-patient surgery: a systematic review and meta-analysis.BMC Anesthesiol. 2018 Nov 8;18(1):162. doi: 10.1186/s12871-018-0632-3. BMC Anesthesiol. 2018. PMID: 30409186 Free PMC article.
-
Anesthesia and Long-term Oncological Outcomes: A Systematic Review and Meta-analysis.Anesth Analg. 2021 Mar 1;132(3):623-634. doi: 10.1213/ANE.0000000000005237. Anesth Analg. 2021. PMID: 33105278
Cited by
-
Frameworks for the design and reporting of anaesthesia interventions in perioperative clinical trials.BJA Open. 2025 Feb 4;13:100374. doi: 10.1016/j.bjao.2024.100374. eCollection 2025 Mar. BJA Open. 2025. PMID: 39991708 Free PMC article.
-
Remimazolam-Based Anesthesia and Systemic Inflammatory Biomarkers in Relation to Postoperative Delirium in Elderly Patients: A Retrospective Cohort Study.Medicina (Kaunas). 2025 May 30;61(6):1023. doi: 10.3390/medicina61061023. Medicina (Kaunas). 2025. PMID: 40572710 Free PMC article.
-
Effects of general versus regional anaesthesia on circadian melatonin rhythm and its association with postoperative delirium in elderly patients undergoing hip fracture surgery: study protocol for a prospective cohort clinical trial.BMJ Open. 2021 Feb 12;11(2):e043720. doi: 10.1136/bmjopen-2020-043720. BMJ Open. 2021. PMID: 33579771 Free PMC article.
-
Anesthetics or anesthetic techniques and cancer surgical outcomes: a possible link.Korean J Anesthesiol. 2021 Jun;74(3):191-203. doi: 10.4097/kja.20679. Epub 2021 Feb 17. Korean J Anesthesiol. 2021. PMID: 33596628 Free PMC article. Review.
-
Anaesthesia by intravenous propofol reduces the incidence of intra-operative gastric electrical slow-wave dysrhythmias compared to isoflurane.Sci Rep. 2023 Jul 21;13(1):11824. doi: 10.1038/s41598-023-38612-w. Sci Rep. 2023. PMID: 37479717 Free PMC article.
References
-
- Diagnostic and statistical manual of mental disorders. Fifth edn Arlington, VA: American Psychiatric Association, 2013.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical