

Postpartum management of hypertensive disorders of pregnancy: a systematic review
- PMID: 29187414
- PMCID: PMC5719299
- DOI: 10.1136/bmjopen-2017-018696
Postpartum management of hypertensive disorders of pregnancy: a systematic review
Abstract
Objectives: Hypertensive disorders of pregnancy (HDP) affect one in ten pregnancies and often persist postpartum when complications can occur. We aimed to determine the effectiveness and safety of pharmacological interventions, other interventions and different care models for postpartum hypertension management.
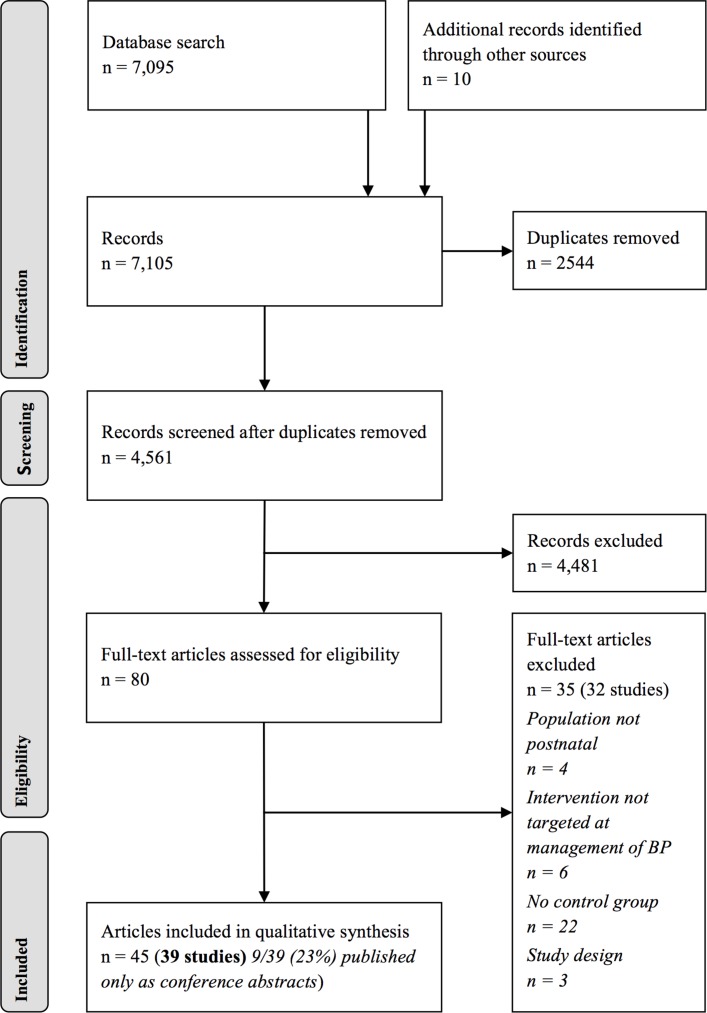
Design: A systematic review was undertaken. Nine electronic databases, including Medline, were searched from inception to 16 March 2017. After duplicate removal, 4561 records were screened. Two authors independently selected studies, extracted study characteristics and data, and assessed methodological quality.
Setting: Randomised controlled trials, case-control studies and cohort studies from any country and healthcare setting.
Participants: Postnatal women with HDP.
Interventions: Therapeutic intervention for management of hypertension, compared with another intervention, placebo or no intervention.
Primary and secondary outcome measures: Outcome data were collected for maternal mortality and severe morbidity; systolic, diastolic and mean arterial blood pressure (BP) control; and safety data. Secondary outcome data collected included the length of postnatal hospital stay and laboratory values.
Results: 39 studies were included (n=2901). Results were heterogeneous in terms of intervention, comparison and outcome requiring a narrative approach. There were insufficient data to recommend any single pharmacological intervention. 18 studies reported calcium-channel blockers, vasodilators and beta-blockers lowered BP postpartum. 12 of these reported safety data. Limited data existed regarding management in the weeks following hospital discharge. Neither loop diuretics (three studies) nor corticosteroids (one study) produced clinical benefit. Uterine curettage significantly reduced BP over the first 48 hours postpartum (range 6-13 mm Hg) compared with standard care (eight studies), with safety data only reported by four of eight studies.
Conclusion: There was insufficient evidence to recommend a particular BP threshold, agent or model of care, but three classes of antihypertensive appeared variably effective. Further comparative research, including robust safety data, is required. Curettage reduced BP, but without adequate reporting of harms, so it cannot currently be recommended.
Keywords: antihypertensive medication; gestational hypertension; hypertensive disorders of pregnancy; postpartum; preeclampsia; systematic review.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Epidural therapy for the treatment of severe pre-eclampsia in non labouring women.Cochrane Database Syst Rev. 2017 Nov 28;11(11):CD009540. doi: 10.1002/14651858.CD009540.pub2. Cochrane Database Syst Rev. 2017. PMID: 29181841 Free PMC article.
-
Beta-blockers for hypertension.Cochrane Database Syst Rev. 2007 Jan 24;(1):CD002003. doi: 10.1002/14651858.CD002003.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2012 Aug 15;(8):CD002003. doi: 10.1002/14651858.CD002003.pub3. PMID: 17253471 Updated.
-
Oral beta-blockers for mild to moderate hypertension during pregnancy.Cochrane Database Syst Rev. 2000;2003(4):CD002863. doi: 10.1002/14651858.CD002863. Cochrane Database Syst Rev. 2000. Update in: Cochrane Database Syst Rev. 2003;(3):CD002863. doi: 10.1002/14651858.CD002863. PMID: 11034777 Free PMC article. Updated.
-
Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term.Cochrane Database Syst Rev. 2017 Jan 15;1(1):CD009273. doi: 10.1002/14651858.CD009273.pub2. Cochrane Database Syst Rev. 2017. PMID: 28106904 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
Cited by
-
Optimal management of post-discharge postpartum hypertensive disorders of pregnancy: a quality improvement initiative.Obstet Med. 2023 Mar;16(1):29-34. doi: 10.1177/1753495X221074613. Epub 2022 Feb 10. Obstet Med. 2023. PMID: 37139511 Free PMC article.
-
Oral labetalol versus oral nifedipine for the management of postpartum hypertension a randomized control trial.Pak J Med Sci. 2019 Sep-Oct;35(5):1428-1433. doi: 10.12669/pjms.35.5.812. Pak J Med Sci. 2019. PMID: 31489020 Free PMC article.
-
Pregnancy hypertension diagnosis and care in COVID-19 era and beyond.Ultrasound Obstet Gynecol. 2020 Jul;56(1):7-10. doi: 10.1002/uog.22115. Ultrasound Obstet Gynecol. 2020. PMID: 32506723 Free PMC article. No abstract available.
-
Postpartum Management of Hypertensive Disorders of Pregnancy in Six Large U.S. Hospital Systems: Descriptive Review and Identification of Clinical and Research Gaps.Am J Perinatol. 2025 Aug;42(11):1371-1380. doi: 10.1055/a-2416-5974. Epub 2024 Oct 10. Am J Perinatol. 2025. PMID: 39389559 Review.
-
A Postpartum Remote Hypertension Monitoring Protocol Implemented at the Hospital Level.Obstet Gynecol. 2019 Oct;134(4):685-691. doi: 10.1097/AOG.0000000000003479. Obstet Gynecol. 2019. PMID: 31503166 Free PMC article.
References
-
- Watson DL, Sibai BM, Shaver DC, et al. . Late postpartum eclampsia: an update. South Med J 1983;76:1487–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical