

Mutational Landscape of cfDNA Identifies Distinct Molecular Features Associated With Therapeutic Response to First-Line Platinum-Based Doublet Chemotherapy in Patients with Advanced NSCLC
- PMID: 29187901
- PMCID: PMC5706097
- DOI: 10.7150/thno.21687
Mutational Landscape of cfDNA Identifies Distinct Molecular Features Associated With Therapeutic Response to First-Line Platinum-Based Doublet Chemotherapy in Patients with Advanced NSCLC
Abstract
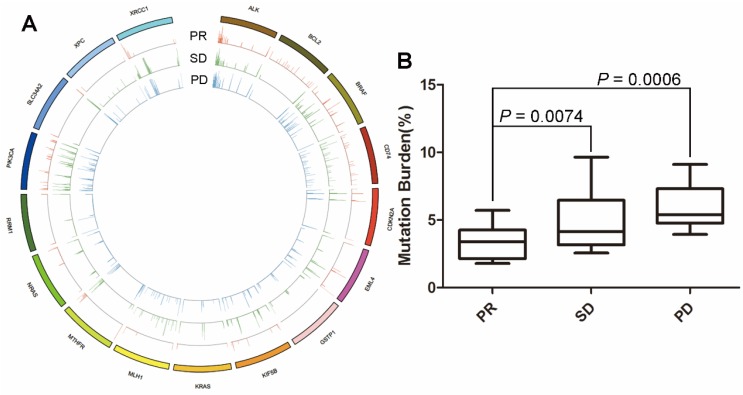
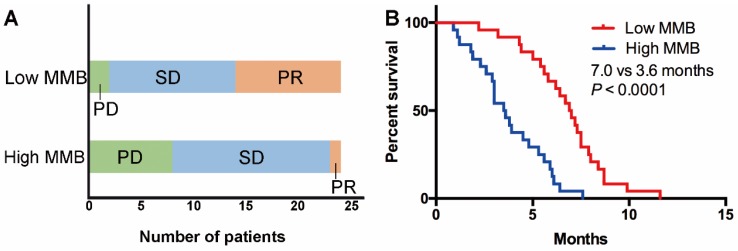
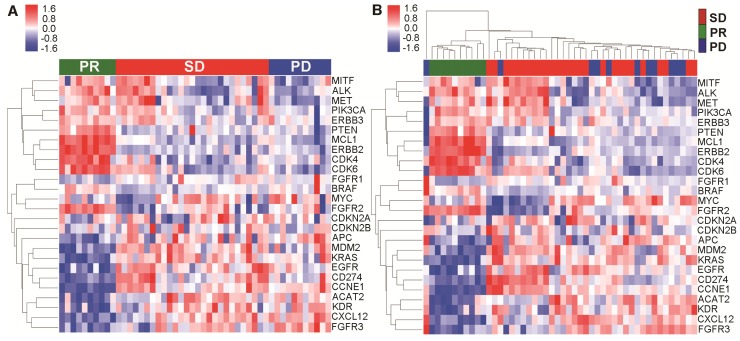
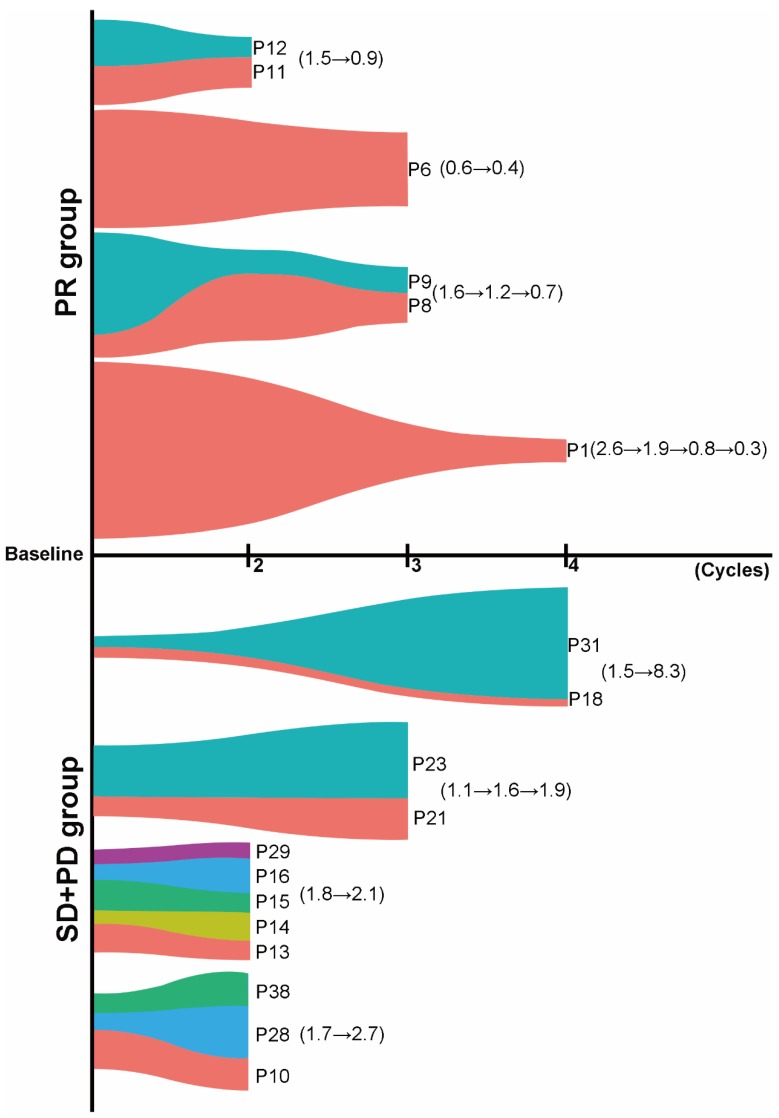
Rationale To investigate whether the mutational landscape of circulating cell-free DNA (cfDNA) could predict and dynamically monitor the response to first-line platinum-based chemotherapy in patients with advanced non-small-cell lung cancer (NSCLC). Methods Eligible patients were included and blood samples were collected from a phase III trial. Both cfDNA fragments and fragmented genomic DNA were extracted for enrichment in a 1.15M size panel covering exon regions of 1,086 genes. Molecular mutational burden (MMB) was calculated to investigate the relationship between molecular features of cfDNA and response to chemotherapy. Results In total, 52 eligible cases were enrolled and their blood samples were prospectively collected at baseline, every cycle of chemotherapy and time of disease progression. At baseline, alterations of 17 genes were found. Patients with partial response (PR) had significantly lower baseline MMB of these genes than those patients with either stable disease (SD) (P = 0.0006) or progression disease (PD) (P = 0.0074). Further analysis revealed that the mutational landscape of cfDNA from pretreatment blood samples were distinctly different among patients with PR vs. SD/PD. For patients with baseline TP53 mutation, those with PR experienced a significant reduction in MMB whereas patients with SD or PD experienced an increase after two, three or four cycles of chemotherapy. Furthermore, patients with low MMB had superior response rate and significantly longer progression-free survival than those with high MMB. Conclusion This study indicated that the mutational landscape of cfDNA has potential clinical value to predict the therapeutic response to first-line platinum-based doublet chemotherapy in NSCLC patients. At the single gene level, dynamic change of molecular mutational burden of TP53 is valuable to monitor efficacy (and, therefore, might aid in early recognition of resistance and relapse) in patients harboring this mutation at baseline.
Keywords: Non-small-cell lung cancer; chemotherapy; circulating cell-free DNA; molecular mutational burden.
Conflict of interest statement
Competing Interests: Wenbo Han, Jianfei Wang, Henghui Zhang and Bo Du are employees of Beijing Genecast Biotechnology Co., Beijing, China. The other authors declare no potential conflict of interest.
Figures
References
-
- Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C. et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–42. - PubMed
-
- Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A. et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016;375:1823–1833. - PubMed
-
- Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T. et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371:2167–77. - PubMed
-
- Tan WL, Jain A, Takano A, Newell EW, Iyer NG, Lim WT. et al. Novel therapeutic targets on the horizon for lung cancer. Lancet Oncol. 2016;17:e347–62. - PubMed
-
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Cancer statistics in China, 2015. CA Cancer J Clin; 2016. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
