

The endoscopic endonasal approach to cranio-cervical junction: the complete panel
- PMID: 29187946
- PMCID: PMC5660904
- DOI: 10.11604/pamj.2017.27.277.12220
The endoscopic endonasal approach to cranio-cervical junction: the complete panel
Abstract
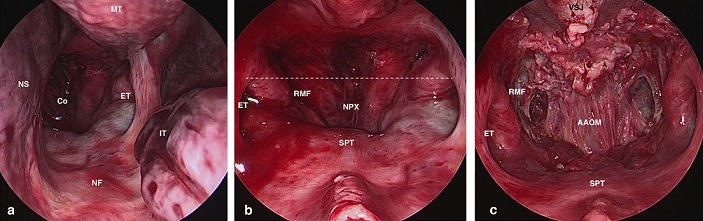
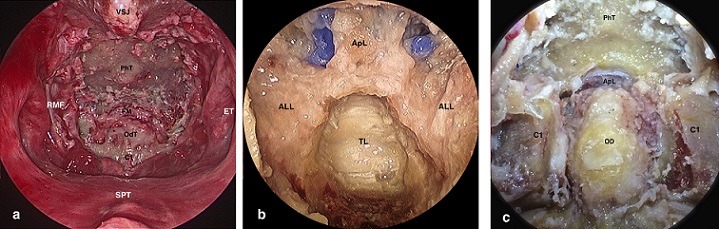
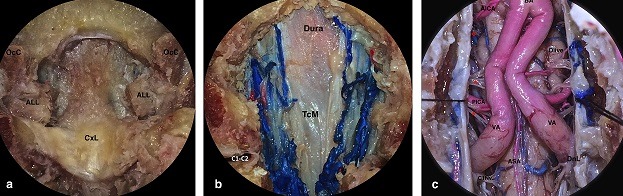
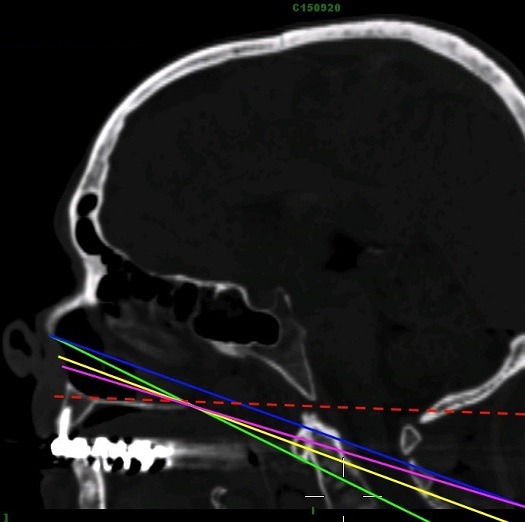
We aim to establish a complete summary on the Endoscopic Endonasal Approach (EEA) to Cranio Cervical Junction (CCJ): evolution since first description, criteria to predict the feasibility and limitations, anatomical landmarks, indications and biomechanical evaluation after performing the approach. A comprehensive literature search to identify all available literature published between March 2002 and June 2015, the articles were divided into four categories according to their main purpose: 1- surgical technique, 2- anatomical landmarks and limitations, 3- literature reviews to identify main indications, 4- biomechanical studies. Thereafter, we demonstrate the approach step-by-step, using 1 fresh and 3 silicon injected embalmed cadaveric specimen heads. 61 articles and one poster were identified. The approach was first described on cadaveric study in 2002, and firstly used to perform odontoidectomy in 2005. The main indication is odontoid rheumatoid pannus and basilar invagination. The nasopalatine line (NPL), the superior nostril-hard palate Line (SN-HP), the naso-axial line (NAxL), the rhinopalatine Line (RPL) and other methods were described to predict the anatomical feasibility of the approach. The craniocervical fusion is potentially unnecessary after removal of < 75% of one occipital condyle. A recent cadaveric study stated the possibility of C1-C2 fusion via EEA. This paper reviews all available clinical and anatomical studies on the EEA to CCJ. The approach marked a significant evolution since its first description in 2002. Because of its lesser complications compared to the transoral approach, the EEA became when feasible, the approach of choice to the ventral CCJ.
Keywords: Craniocervical junction; endonasal; endoscopic; odontoidectomy; transnasal.
Figures
References
-
- Apuzzo ML, Weiss MH, Heiden JS. Transoral exposure of the atlantoaxial region. Neurosurgery. 1978;3(2):201–7. - PubMed
-
- Crockard HA, Calder I, Ransford AO. One-stage transoral decompression and posterior fixation in rheumatoid atlanto-axial subluxation. J Bone Joint Surg Br. 1990;72(4):682–5. - PubMed
-
- Dickman CA, Locantro J, Fessler RG. The influence of transoral odontoid resection on stability of the craniovertebral junction. J Neurosurg. 1992;77(4):525–30. - PubMed
-
- Frempong-Boadu AK, Faunce WA, Fessler RG. Endoscopically assisted transoral-transpharyngeal approach to the craniovertebral junction. Neurosurgery. 2002;51(5):60–6. - PubMed
-
- Menezes AH, VanGilder JC. Transoral-transpharyngeal approach to the anterior craniocervical junction: ten-year experience with 72 patients. J Neurosurg. 1988;69(6):895–903. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
