

Scaling-up primary health care-based prevention and management of heavy drinking at the municipal level in middle-income countries in Latin America: Background and protocol for a three-country quasi-experimental study
- PMID: 29188013
- PMCID: PMC5686480
- DOI: 10.12688/f1000research.11173.3
Scaling-up primary health care-based prevention and management of heavy drinking at the municipal level in middle-income countries in Latin America: Background and protocol for a three-country quasi-experimental study
Abstract
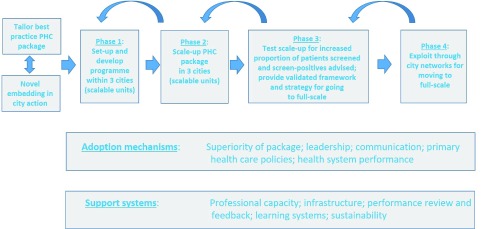
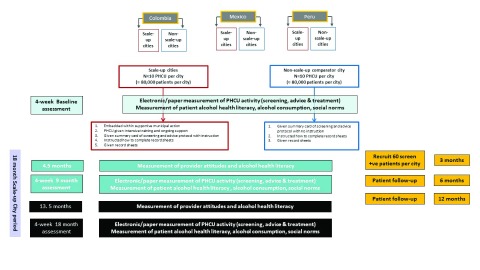
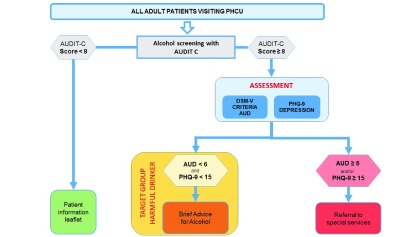
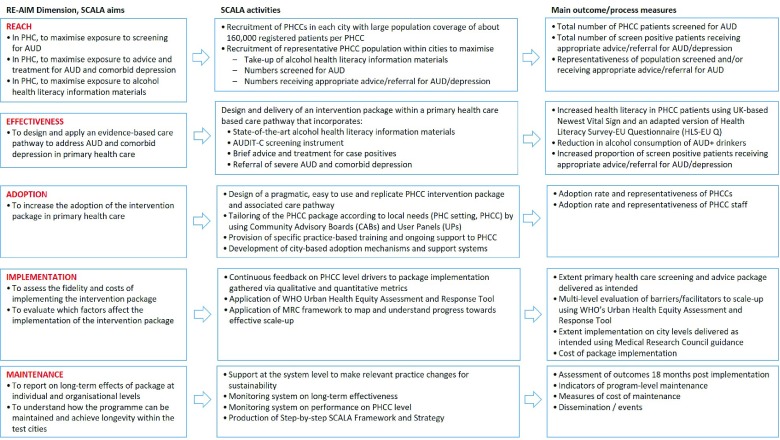
Background: While primary health care (PHC)-based prevention and management of heavy drinking is clinically effective and cost-effective, it remains poorly implemented in routine practice. Systematic reviews and multi-country studies have demonstrated the ability of training and support programmes to increase PHC-based screening and brief advice activity to reduce heavy drinking. However, gains have been only modest and short term at best. WHO studies have concluded that a more effective uptake could be achieved by embedding PHC activity within broader community and municipal support. Protocol: A quasi-experimental study will compare PHC-based prevention and management of heavy drinking in three intervention cities from Colombia, Mexico and Peru with three comparator cities from the same countries. In the implementation cities, primary health care units (PHCUs) will receive training embedded within ongoing supportive municipal action over an 18-month implementation period. In the comparator cities, practice as usual will continue at both municipal and PHCU levels. The primary outcome will be the proportion of consulting adult patients intervened with (screened and advice given to screen positives). The study is powered to detect a doubling of the outcome measure from an estimated 2.5/1,000 patients at baseline. Formal evaluation points will be at baseline, mid-point and end-point of the 18-month implementation period. We will present the ratio (plus 95% confidence interval) of the proportion of patients receiving intervention in the implementation cities with the proportions in the comparator cities. Full process evaluation will be undertaken, coupled with an analysis of potential contextual, financial and political-economy influencing factors. Discussion: This multi-country study will test the extent to which embedding PHC-based prevention and management of alcohol use disorder with supportive municipal action leads to improved scale-up of more patients with heavy drinking receiving appropriate advice and treatment. Study status: The four-year study will start on 1 st December 2017.
Keywords: Scale-up; alcohol use disorder; cities; harmful use of alcohol; heavy drinking; implementation; primary health care; training and support.
Conflict of interest statement
No competing interests were disclosed.
Figures
References
-
- GBD 2015 Risk Factors Collaborators: Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1659–724. 10.1016/S0140-6736(16)31679-8 - DOI - PMC - PubMed
-
- World Health Organization (ICD-10). Reference Source
-
- World Health Organization (ICD-11). Reference Source
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Washington, DC, American Psychiatric Association.2013. Reference Source
LinkOut - more resources
Full Text Sources
Other Literature Sources