

Response of Leptomeningeal Dissemination of Anaplastic Glioma to Temozolomide: Experience of Two Cases
- PMID: 29188211
- PMCID: PMC5700034
- DOI: 10.14791/btrt.2017.5.2.99
Response of Leptomeningeal Dissemination of Anaplastic Glioma to Temozolomide: Experience of Two Cases
Abstract
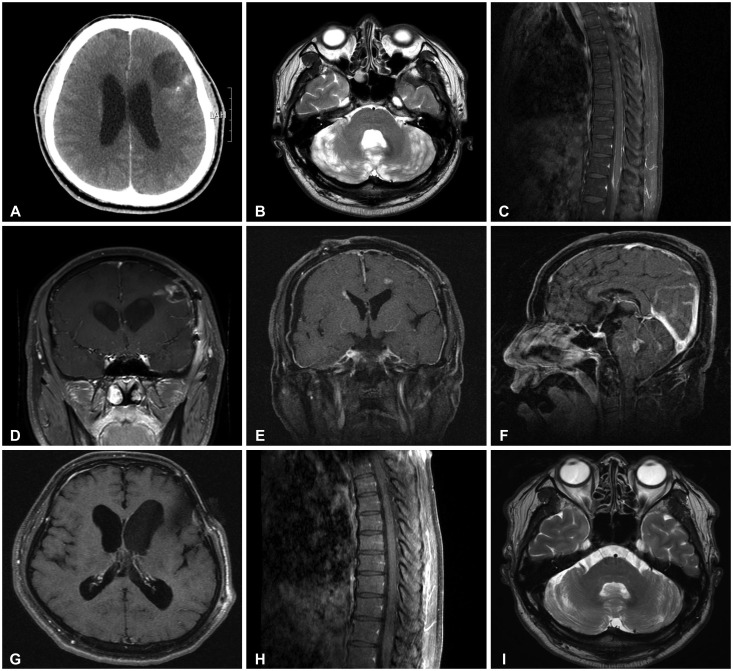
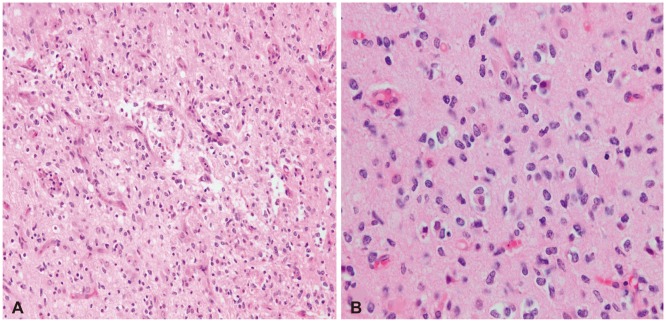
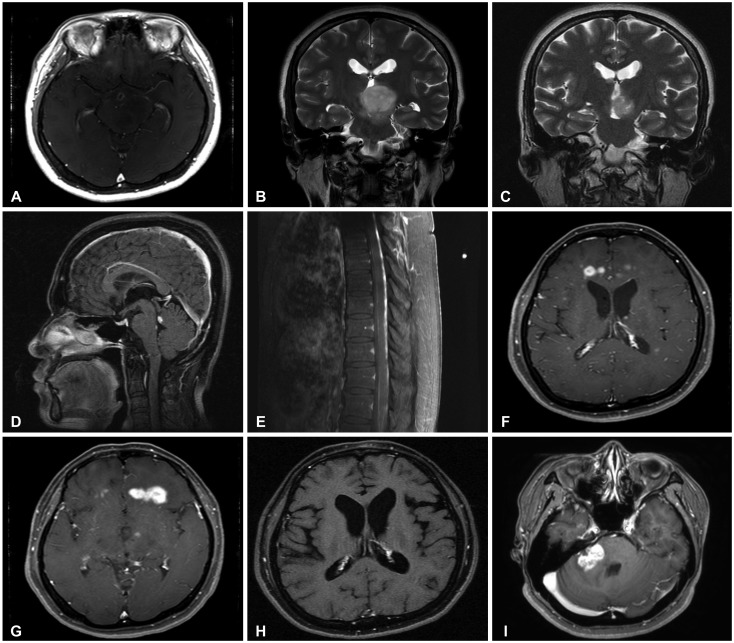
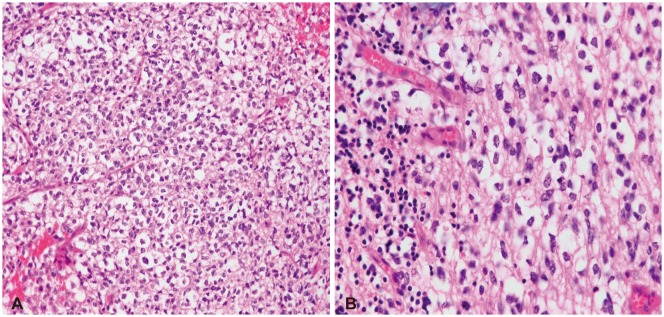
The incidence of leptomeningeal dissemination (LMD) of anaplastic glioma has been increasing. LMD can be observed at the time of initial presentation or the time of recurrence. As a result of both rarity and unusual presentation, a standard therapy has not yet been suggested. In contrast to leptomeningeal carcinomatosis for systemic solid cancers, a relatively prolonged survival is observed in some patients with LMD of anaplastic gliomas. Treatment modalities include whole craniospinal irradiation, intra-cerebrospinal fluid (CSF) chemotherapy, and systemic chemotherapy. In some cases, response to temozolomide (TMZ), with or without combined radiation has been reported. Here, we report two cases of LMD of an anaplastic glioma. In one case LMD presented at the time of diagnosis, and in the other at the time of recurrence after radiation. CSF cytology was positive in both cases, and persisted in spite of intrathecal methotrexate chemotherapy. Later, TMZ was prescribed for progressing brain parenchymal lesions, and both radiological and cytological responses were obtained after oral TMZ treatment.
Keywords: Cerebrospinal fluid; Drug effect; Leptomeningeal carcinomatosis; Malignant glioma; Temozolomide.
Conflict of interest statement
Conflicts of Interest: The authors have no financial conflicts of interest.
Figures
Similar articles
-
Efficacy of temozolomide and bevacizumab for the treatment of leptomeningeal dissemination of recurrent glioblastoma: A case report.Oncol Lett. 2015 Apr;9(4):1885-1888. doi: 10.3892/ol.2015.2940. Epub 2015 Feb 6. Oncol Lett. 2015. PMID: 25789061 Free PMC article.
-
The clinical features of spinal leptomeningeal dissemination from malignant gliomas.J Korean Neurosurg Soc. 2011 Jun;49(6):334-8. doi: 10.3340/jkns.2011.49.6.334. Epub 2011 Jun 30. J Korean Neurosurg Soc. 2011. PMID: 21887390 Free PMC article.
-
Cyberknife Radiosurgery and Concurrent Intrathecal Chemotherapy for Leptomeningeal Metastases: Case Report of Prolonged Survival of a HER-2+ Breast Cancer Patient Status-Post Craniospinal Irradiation.Cureus. 2016 Jan 7;8(1):e453. doi: 10.7759/cureus.453. Cureus. 2016. PMID: 26918221 Free PMC article.
-
Leptomeningeal Metastasis: A Review of the Pathophysiology, Diagnostic Methodology, and Therapeutic Landscape.Curr Oncol. 2023 Jun 19;30(6):5906-5931. doi: 10.3390/curroncol30060442. Curr Oncol. 2023. PMID: 37366925 Free PMC article. Review.
-
Leptomeningeal Disease: Current Approaches and Future Directions.Curr Neurol Neurosci Rep. 2025 Mar 18;25(1):25. doi: 10.1007/s11910-025-01412-y. Curr Neurol Neurosci Rep. 2025. PMID: 40100294 Free PMC article. Review.
Cited by
-
Leptomeningeal Metastasis in Gliomas : Clinical Characteristics and Risk Factors.J Korean Neurosurg Soc. 2023 Jul;66(4):465-475. doi: 10.3340/jkns.2022.0166. Epub 2022 Dec 12. J Korean Neurosurg Soc. 2023. PMID: 36503217 Free PMC article.
-
Long-Term Remission of Recurrent Anaplastic Oligodendroglioma With WT-1-Specific CD8+ T-Cell Therapy: A Case Report.Brain Tumor Res Treat. 2025 Apr;13(2):65-72. doi: 10.14791/btrt.2025.0010. Brain Tumor Res Treat. 2025. PMID: 40347129 Free PMC article.
-
A Retrospective Study on Spinal Dissemination of Supratentorial Glioma.Front Oncol. 2021 Dec 22;11:765399. doi: 10.3389/fonc.2021.765399. eCollection 2021. Front Oncol. 2021. PMID: 35004286 Free PMC article.
References
-
- Saito R, Kumabe T, Jokura H, Shirane R, Yoshimoto T. Symptomatic spinal dissemination of malignant astrocytoma. J Neurooncol. 2003;61:227–235. - PubMed
-
- Michotte A, Chaskis C, Sadones J, Veld PI, Neyns B. Primary leptomeningeal anaplastic oligodendroglioma with a 1p36-19q13 deletion: report of a unique case successfully treated with Temozolomide. J Neurol Sci. 2009;287:267–270. - PubMed
-
- Ostermann S, Csajka C, Buclin T, et al. Plasma and cerebrospinal fluid population pharmacokinetics of temozolomide in malignant glioma patients. Clin Cancer Res. 2004;10:3728–3736. - PubMed
-
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016;131:803–820. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
