

Epidemiology, biology and therapy of Merkel cell carcinoma: conclusions from the EU project IMMOMEC
- PMID: 29188306
- PMCID: PMC6015651
- DOI: 10.1007/s00262-017-2099-3
Epidemiology, biology and therapy of Merkel cell carcinoma: conclusions from the EU project IMMOMEC
Abstract
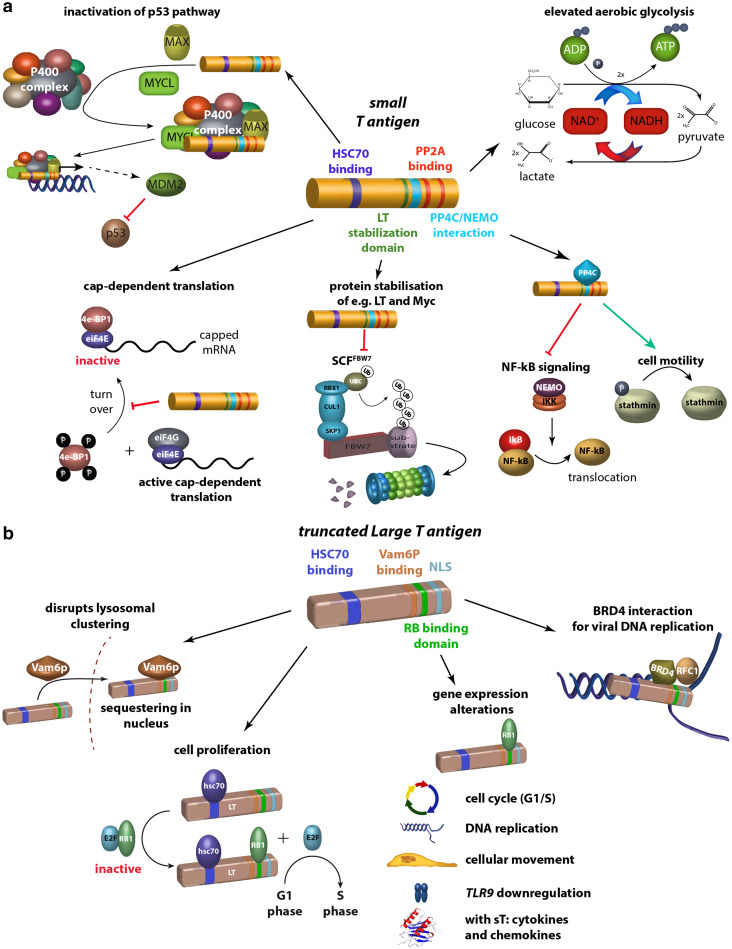
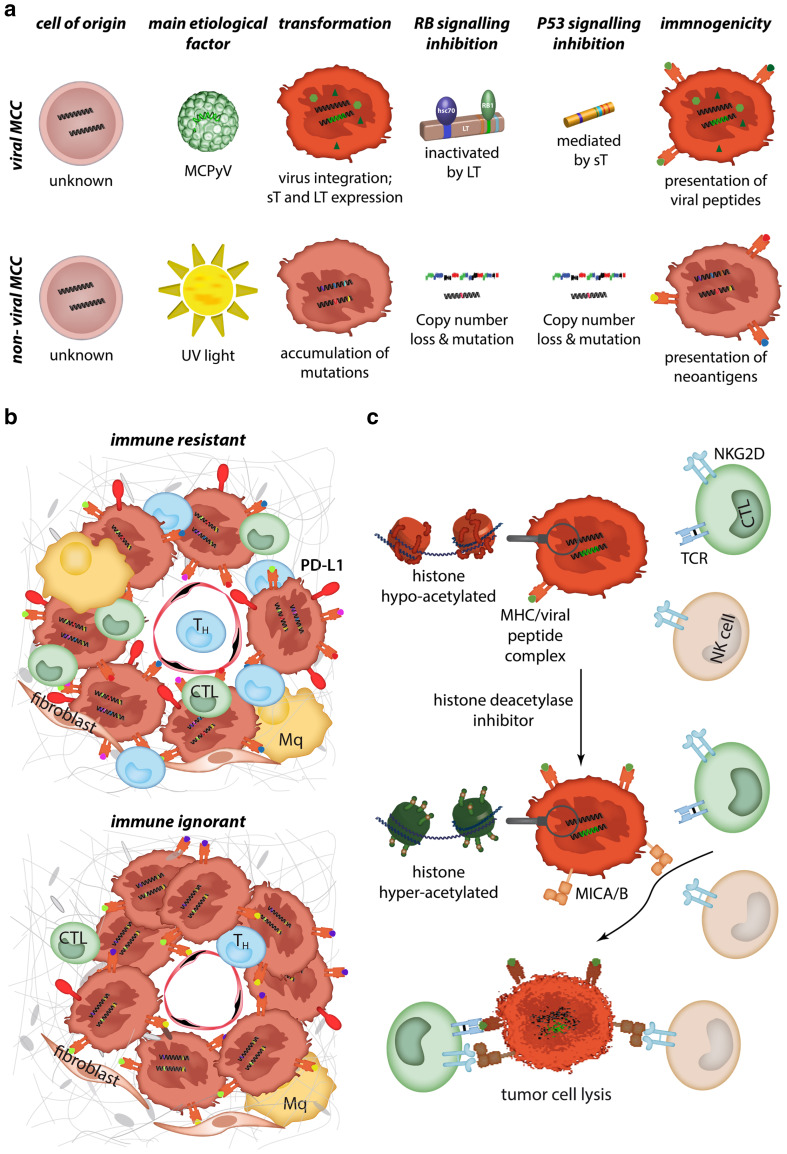
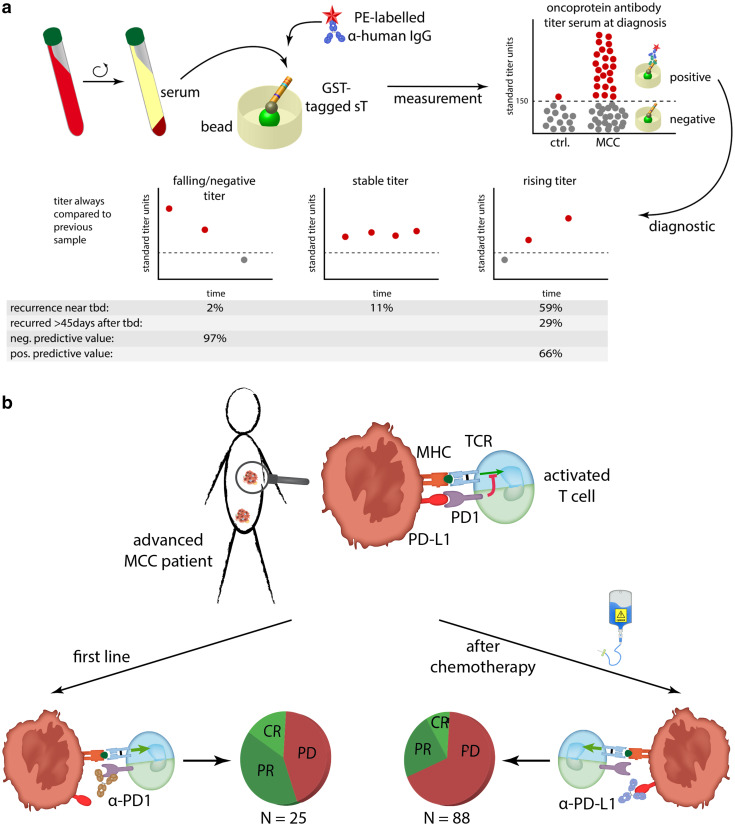
Merkel cell carcinoma (MCC) is a highly aggressive, often lethal neuroendocrine cancer. Its carcinogenesis may be either caused by the clonal integration of the Merkel cell polyomavirus into the host genome or by UV-induced mutations. Notably, virally-encoded oncoproteins and UV-induced mutations affect comparable signaling pathways such as RB restriction of cell cycle progression or p53 inactivation. Despite its low incidence, MCC recently received much attention based on its exquisite immunogenicity and the resulting major success of immune modulating therapies. Here, we summarize current knowledge on epidemiology, biology and therapy of MCC as conclusion of the project 'Immune Modulating strategies for treatment of Merkel Cell Carcinoma', which was funded over a 5-year period by the European Commission to investigate innovative immunotherapies for MCC.
Keywords: Cell of origin; Epidemiology; IMMOMEC; Immunotherapy; Merkel cell carcinoma; Merkel cell polyomavirus.
Conflict of interest statement
J. C. Becker has received speaker honoraria from Amgen, MerckSerono, and Pfizer, advisory board honoraria from Amgen, CureVac, eTheRNA, Lytix, MerckSerono, Novartis, Rigontec, and Takeda as well as research funding from Boehringer Ingelheim, BMS and MerckSerono; the activities with BMS, MerckSerono and Pfizer are related to the submitted report (therapy of advanced MCC). A research project in J. A. DeCaprio’s laboratory is supported by Constellation Pharmaceuticals. P. Nghiem has served as a consultant for EMD Serono and Pfizer and has received research support to his institution from Bristol-Myers Squibb. The other authors declare that they have no conflict of interest.
Figures
Similar articles
-
Update on Merkel Cell Carcinoma.Clin Lab Med. 2017 Sep;37(3):485-501. doi: 10.1016/j.cll.2017.05.004. Epub 2017 Jun 13. Clin Lab Med. 2017. PMID: 28802497 Review.
-
Advances in Immunotherapy for Metastatic Merkel Cell Carcinoma: A Clinician's Guide.J Natl Compr Canc Netw. 2018 Jun;16(6):782-790. doi: 10.6004/jnccn.2018.7049. J Natl Compr Canc Netw. 2018. PMID: 29891528 Review.
-
Immunobiology of Merkel cell carcinoma: implications for immunotherapy of a polyomavirus-associated cancer.Curr Oncol Rep. 2011 Dec;13(6):488-97. doi: 10.1007/s11912-011-0197-5. Curr Oncol Rep. 2011. PMID: 21953511 Free PMC article. Review.
-
Scientific and clinical developments in Merkel cell carcinoma: A polyomavirus-driven, often-lethal skin cancer.J Dermatol Sci. 2022 Jan;105(1):2-10. doi: 10.1016/j.jdermsci.2021.10.004. Epub 2021 Oct 18. J Dermatol Sci. 2022. PMID: 34836718 Free PMC article. Review.
-
Merkel cell carcinoma - recent advances in the biology, diagnostics and treatment.Int J Biochem Cell Biol. 2014 Aug;53:536-46. doi: 10.1016/j.biocel.2014.04.023. Epub 2014 May 5. Int J Biochem Cell Biol. 2014. PMID: 24811434 Review.
Cited by
-
Multimodal Strategy in Localized Merkel Cell Carcinoma: Where Are We and Where Are We Heading?Int J Mol Sci. 2021 Sep 30;22(19):10629. doi: 10.3390/ijms221910629. Int J Mol Sci. 2021. PMID: 34638968 Free PMC article. Review.
-
Merkel cell carcinoma of the eyelid and periocular region: A review.Saudi J Ophthalmol. 2022 Apr 18;35(3):186-192. doi: 10.4103/SJOPT.SJOPT_55_21. eCollection 2021 Jul-Sep. Saudi J Ophthalmol. 2022. PMID: 35601863 Free PMC article.
-
Is the Addition of Chemotherapy to Adjuvant Radiation in Merkel Cell Cancer Beneficial? Real-World Data with Long-Term Follow-Up.Cancers (Basel). 2025 Mar 11;17(6):945. doi: 10.3390/cancers17060945. Cancers (Basel). 2025. PMID: 40149282 Free PMC article.
-
Merkel Cell Polyomavirus T Antigens Induce Merkel Cell-Like Differentiation in GLI1-Expressing Epithelial Cells.Cancers (Basel). 2020 Jul 21;12(7):1989. doi: 10.3390/cancers12071989. Cancers (Basel). 2020. PMID: 32708246 Free PMC article.
-
Merkel Cell Polyomavirus (MCPyV) and Cancers: Emergency Bell or False Alarm?Cancers (Basel). 2022 Nov 11;14(22):5548. doi: 10.3390/cancers14225548. Cancers (Basel). 2022. PMID: 36428641 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
