

Late-Life Body Mass Index, Rapid Weight Loss, Apolipoprotein E ε4 and the Risk of Cognitive Decline and Incident Dementia
- PMID: 29188888
- PMCID: PMC5736008
- DOI: 10.1007/s12603-017-0906-3
Late-Life Body Mass Index, Rapid Weight Loss, Apolipoprotein E ε4 and the Risk of Cognitive Decline and Incident Dementia
Abstract
Objectives: To examine the effect of late-life body mass index (BMI) and rapid weight loss on incident mild cognitive impairment (MCI) and Alzheimer's disease (AD).
Design: Prospective longitudinal cohort study.
Setting: National Alzheimer's Coordinating Center (NACC) Uniform Data Set, including 34 past and current National Institute on Aging-funded AD Centers across the United States.
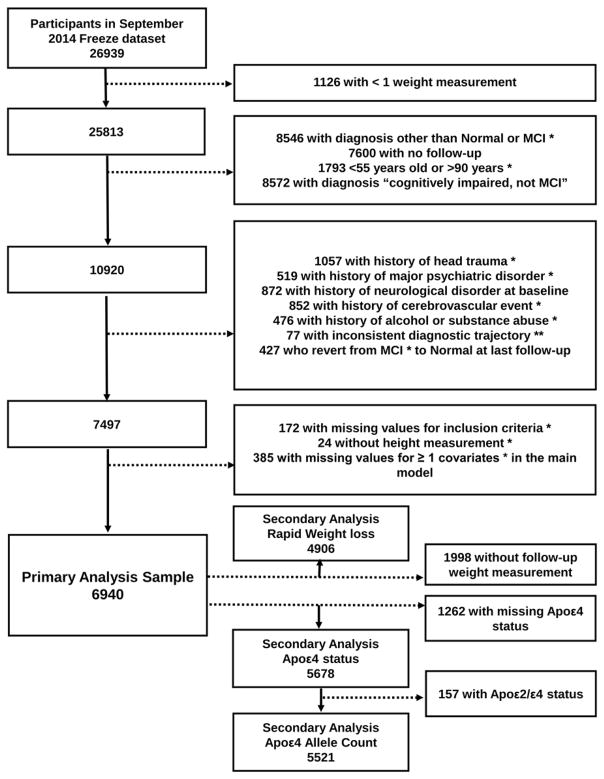
Participants: 6940 older adults (n=5061 normal cognition [NC]; n=1879 MCI).
Measurements: BMI (kg/m2) and modified Framingham Stroke Risk Profile (FSRP) score (sex, age, systolic blood pressure, anti-hypertension medication, diabetes mellitus, cigarette smoking, prevalent cardiovascular disease, atrial fibrillation) were assessed at baseline. Cognition and weight were assessed annually.
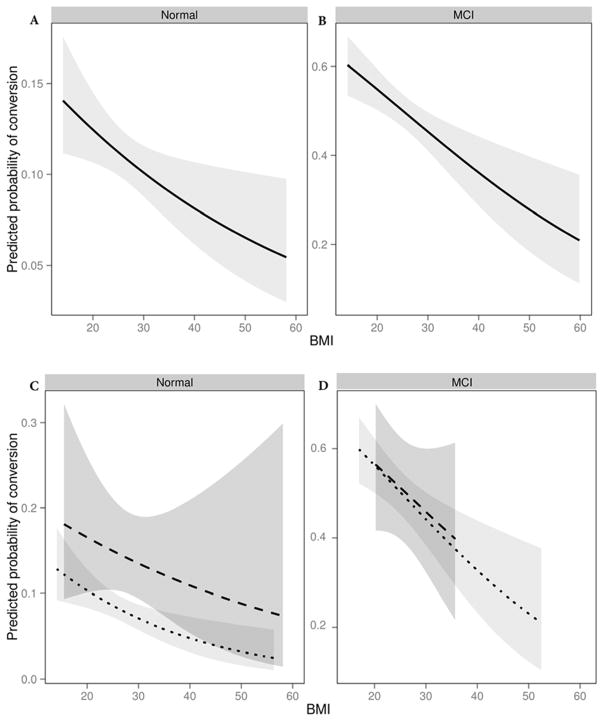
Results: Multivariable binary logistic regression, adjusting for age, sex, race, education, length of follow-up, and modified FSRP related late-life BMI to risk of diagnostic conversion from NC to MCI or AD and from MCI to AD. Secondary analyses related late-life BMI to diagnostic conversion in the presence of rapid weight loss (>5% decrease in 12 months) and apolipoprotein E (APOE) ε4. During a mean 3.8-year follow-up period, 12% of NC participants converted to MCI or AD and 49% of MCI participants converted to AD. Higher baseline BMI was associated with a reduced probability of diagnostic conversion, such that for each one-unit increase in baseline BMI there was a reduction in diagnostic conversion for both NC (OR=0.977, 95%CI 0.958-0.996, p=0.015) and MCI participants (OR=0.962, 95%CI 0.942-0.983, p<0.001). The protective effect of higher baseline BMI did not persist in the setting of rapid weight loss but did persist when adjusting for APOE ε4.
Conclusions: Higher late-life BMI is associated with a lower risk of incident MCI and AD but is not protective in the presence of rapid weight loss.
Keywords: Alzheimer’s disease; Dementia; body mass index; cognition; frailty.
Conflict of interest statement
None for all authors.
Figures
References
-
- Yaffe K, Lindquist K, Vittinghoff E, Barnes D, Simonsick EM, Newman A, Satterfield S, Rosano C, Rubin SM, Ayonayon HN, et al. The effect of maintaining cognition on risk of disability and death. Journal of the American Geriatrics Society. 2010;58(5):889–94. doi: 10.1111/j.1532-5415.2010.02818.x. - DOI - PMC - PubMed
-
- Sandman PO, Adolfsson R, Nygren C, Hallmans G, Winblad B. Nutritional status and dietary intake in institutionalized patients with Alzheimer’s disease and multiinfarct dementia. Journal of the American Geriatrics Society. 1987;35(1):31–8. - PubMed
-
- White H, Pieper C, Schmader K. The association of weight change in Alzheimer’s disease with severity of disease and mortality: a longitudinal analysis. Journal of the American Geriatrics Society. 1998;46(10):1223–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AG013854/AG/NIA NIH HHS/United States
- P50 AG005142/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- P50 AG025688/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- K23 AG045966/AG/NIA NIH HHS/United States
- P30 AG028383/AG/NIA NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- P50 AG005131/AG/NIA NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- P50 AG005146/AG/NIA NIH HHS/United States
- P30 AG035982/AG/NIA NIH HHS/United States
- P50 AG008702/AG/NIA NIH HHS/United States
- K23 AG048347/AG/NIA NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- P30 AG008051/AG/NIA NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- R01 HL111516/HL/NHLBI NIH HHS/United States
- P30 AG013846/AG/NIA NIH HHS/United States
- P50 AG005136/AG/NIA NIH HHS/United States
- P30 AG012300/AG/NIA NIH HHS/United States
- U54 HD083211/HD/NICHD NIH HHS/United States
- P50 AG016573/AG/NIA NIH HHS/United States
- P50 AG016570/AG/NIA NIH HHS/United States
- P50 AG005134/AG/NIA NIH HHS/United States
- P30 AG008017/AG/NIA NIH HHS/United States
- P50 AG005138/AG/NIA NIH HHS/United States
- K12 HD043483/HD/NICHD NIH HHS/United States
- K01 AG049164/AG/NIA NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
- P30 AG019610/AG/NIA NIH HHS/United States
- K24 AG046373/AG/NIA NIH HHS/United States
- P50 AG033514/AG/NIA NIH HHS/United States
- R01 AG034962/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
